Update
At vero eos et accusamus et iusto odio dignissimos ducimus qui blanditiis praesentium voluptatum deleniti atque corrupti quos dolores et quas molestias excepturi sint occaecati cupiditate non provident, similique sunt in culpa qui officia deserunt mollitia animi, id est laborum et dolorum fuga. Et harum quidem rerum facilis est et expedita distinctio. Nam libero tempore, cum soluta nobis est eligendi optio cumque nihil impedit quo minus id quod maxime placeat facere possimus, omnis voluptas assumenda est, omnis dolor repellendus. Temporibus autem quibusdam et aut officiis debitis aut rerum necessitatibus saepe eveniet ut et voluptates repudiandae sint et molestiae non recusandae. Itaque earum rerum hic tenetur a sapiente delectus, ut aut reiciendis voluptatibus maiores alias consequatur aut perferendis doloribus asperiores repellat.
Summary
The treatment of ostial stenosis by percutaneous techniques has been associated with lower procedural success rates, more frequent in-hospital complications and a greater likelihood of restenosis when compared with non-ostial stenoses. While indications for PCI of ostial lesions, in principle, follow the same considerations as those for other coronary lesions, namely, lesion assessment, material selection and interventional strategy, a precise knowledge of the anatomy and physiology of ostial lesions is required to obtain the best possible interventional result.
Ostial lesions are frequently rigid and heavily calcified, which may lead to incomplete stent expansion and thus may require preparation with debulking techniques. Complications prone to occur in ostial lesion PCI include dissections of the vessel (which often are caused by aggressive or unintentional guide catheter manipulation), or, the loss of guide catheter position due to insufficient support.
Specific ostial intervention techniques include the so-called draw-back stent deployment technique and the tail-wire or Szabo-technique. These manoeuvres may be helpful to achieve precise coverage of the ostium without excessive protrusion into the aorta or the respective main vessel.
Introduction
Lesions within 3 mm from the origin of a coronary vessel are classified as ostial lesions. A distinction can be drawn between aorto-ostial and non-aorto-ostial lesions, while some authors also introduce the term branch-ostial lesions for lesions at the ostia of side-branches of coronary vessels [11. Jokhi P, Curzen N. Percutaneous coronary intervention of ostial lesions. EuroIntervention. 2009;5:511-4.
Excellent overview on PCI in ostial lesions. Nicely describes all relevant techniques.]. Ostial lesions in general are frequently found to be fibrotic and calcified [22. Pesenti-Rossi D, Chouli M, Gharbi M, Ghostine S, Habib Y, Brenot P, Angel CY, Paul JF, Capderou A, Lancelin B, Caussin C. Coronary aorto-ostial stenosis analysed by multislice computed tomography: a new tool for percutaneous coronary intervention? EuroIntervention. 2011;6:717-21. ]. Aorto-ostial lesions, namely those at the origin of the left main (LM) and the right coronary artery (RCA), demonstrate particularly high rigidity and recoil due to the density of elastic fibres present in the aortic wall.
While all ostial lesions require the precise handling of interventional tools, the intervention of non-aorto-ostial lesions may be additionally complicated by their branching off from another vessel and thus requiring complex techniques with multiple devices (  View chapter ).
View chapter ).
The treatment of ostial stenoses with balloon angioplasty alone (POBA) has been associated with low procedural success rates, more frequent in-hospital complications and a greater likelihood of restenosis when compared with POBA of non-ostial stenoses [33. Ellis SG, Vandormael MG, Cowley MJ, DiSciascio G, Deligonul U, Topol EJ, Bulle TM. Coronary morphologic and clinical determinants of procedural outcome with angioplasty for multivessel coronary disease. Implications for patient selection. Multivessel Angioplasty Prognosis Study Group. Circulation. 1990;82:1193-202. , 44. Tan KH, Sulke N, Taub N, Sowton E. Percutaneous transluminal coronary angioplasty of aorta ostial, non-aorta ostial, and branch ostialstenoses: acute and long-term outcome. Eur Heart J. 1995;16:631-9. ]. While the introduction of bare metal stents (BMS) led to acceptable procedural results, long-term revascularisation rates were nevertheless still higher than in non-ostial lesions [55. Mavromatis K, Ghazzal Z, Veledar E, Diamandopoulos L, Weintraub WS, Douglas JS, Kalynych AM. Comparison of outcomes of percutaneous coronary intervention of ostial versus nonostial narrowing of the major epicardial coronary arteries. Am J Cardiol. 2004;94:583-7. , 66. Rocha-Singh K, Morris N, Wong SC, Schatz RA, Teirstein PS. Coronary stenting for treatment of ostial stenoses of native coronary arteries or aortocoronary saphenous venous grafts. Am J Cardiol. 1995;75:26-9. ]. These, however, have improved with the advent of drug-eluting stents (DES) [77. Iakovou I, Ge L, Michev I, Sangiorgi GM, Montorfano M, Airoldi F, Chieffo A, Stankovic G, Vitrella G, Carlino M, Corvaja N, Briquori C, Colombo A. Clinical and angiographic outcome after sirolimus-eluting stent implantation in aorto-ostial lesions. J Am Coll Cardiol. 2004;44:967-71.
Early paper on the success of DES in aorto-ostial lesions., 88. Barlis P, Kaplan S, Dimopoulos K, Ferrante G, Di Mario C. Comparison of bare-metal and sirolimus- or paclitaxel-eluting stents for aorto-ostial coronary disease. Cardiology. 2008;111:270-6. ].
Indications for PCI and lesion assessment
The indications for the use of PCI in ostial lesions follow the same considerations as for other coronary lesions; they point to the improvement of symptoms and/or prognosis.
Besides typical symptoms and non-invasive proof of myocardial ischaemia, the haemodynamic relevance of ostial lesions may also be assessed invasively:
a) Guide catheter: aorto-ostial lesions can often be assessed after intubation with a guide catheter. After spasm provoked by the intubation with the catheter has been excluded (e.g., by the use of intracoronary nitrates, smaller diameter catheters or non-selective contrast injection into the coronary sinus), the lack of contrast reflux into the aortic root after injection into the coronary artery is an indicator for a significant lesion. Similarly, a significant aortic pressure drop and/or ventricularisation after co-axial intubation with a guide catheter (without side-holes) indicates haemodynamic relevance.
b) Intravascular ultrasound (IVUS) and fractional flow reserve (FFR): both have been used for the evaluation of non-ostial coronary lesions [99. Nam CW, Yoon HJ, Cho YK, Park HS, Kim H, Hur SH, Kim YN, Chung IS, Koo BK, Tahk SJ, Fearon WF, Kim KB. Outcomes of percutaneous coronary intervention in intermediate coronary artery disease: fractional flow reserve-guided versus intravascular ultrasound-guided. JACC CardiovascInterv. 2010;3:812-7. ] and may be used for ostia lesions as well. In aorto-ostial lesions both FFR and IVUS assessment require guide catheter disengagement to achieve reliable results. For IVUS, however, this manoeuvre may lead to an overestimation of the remaining luminal area due to non-coaxial imaging of the ostium.
c) Quantitative coronary angiography (QCA): while the severity of ostial lesions may be visually overestimated [1010. Koo BK, Park KW, Kang HJ, Cho YS, Chung WY, Youn TJ, Chae IH, Choi DJ, Tahk SJ, Oh BH, Park YB, Kim HS. Physiological evaluation of the provisional side-branch intervention strategy for bifurcation lesions using fractional flow reserve. Eur Heart J. 2008;29:726-32.
Key paper on the need for intervention in non-aorto-ostial lesions.], QCA also presents some difficulties due to the lack of a proximal reference segment. In non-aorto-ostial lesions dedicated QCA software for bifurcation lesions may be used [1111. Holm NR, Højdahl H, Lassen JF, Thuesen L, Maeng M. Quantitative coronary analysis in the Nordic Bifurcation studies. Int J Cardiovasc Imaging. 2011;27:175-80. ].
Indications for ostial PCI and lesion evaluation> Indications:- Unstable angina pectoris
- Other acute coronary syndromes
- Stable, effort induced angina pectoris or dyspnoea (angina equivalent)
- Significant territory of ischaemic myocardium at risk (can be anticipated in aorto-ostial disease)
>Evaluation:- Lack of contrast reflux or significant pressure drop/ventricularisation after intubation with the guide catheter (CAVE: ostial spasm, non co-axial alignment)
- Intravascular ultrasound (IVUS) and fractional flow reserve (FFR) (CAVE: guide catheter disengagement required)
- Quantitative coronary angiograph (QCA) (CAVE: no proximal reference)
Guiding catheter
a) Guide catheter selection: intervention and assessment of aorto-ostial lesions requires catheter disengagement. Thus, catheters with less support (e.g., Judkins shape) or short-tipped designs are preferrable to avoid deep engagement beyond the ostium. Side-hole catheters are frequently used, however, one should be aware that they require the use of continuous IV adenosine infusion for FFR measurements since measurements based on IC bolus injections will not be accurate. In addition, occlusion of blood flow with the catheter tip in the ostial stenosis often remains unrecognised with side-hole catheters due to the lack of observed aortic pressure drop.
The intervention of non-aorto-ostial lesions frequently requires the use of a second wire to protect the main branch of the vessel, or the simultaneous use of balloons or stents, an adequate catheter size should therefore be chosen in accordance with the planned strategy and any anticipated potential complications.
b) Guidewire selection: there is no need to use specific wires other than standard workhorse wires for ostial lesions.
This might change if specific techniques are used or if bifurcations are involved ( View chapter ). The necessity for catheter disengagement and the sometimes forceful handling in tight, calcified ostial stenoses argue against the use of wires with low support or hydrophilic wires as a primary choice, since the former may result in poor stent delivery and use of the latter are prone to causing distal perforation.
c) Stent selection: DES appear to have an advantage over BMS in ostial lesions with respect to lower target lesion revascularisation rates [77. Iakovou I, Ge L, Michev I, Sangiorgi GM, Montorfano M, Airoldi F, Chieffo A, Stankovic G, Vitrella G, Carlino M, Corvaja N, Briquori C, Colombo A. Clinical and angiographic outcome after sirolimus-eluting stent implantation in aorto-ostial lesions. J Am Coll Cardiol. 2004;44:967-71.
Early paper on the success of DES in aorto-ostial lesions., 88. Barlis P, Kaplan S, Dimopoulos K, Ferrante G, Di Mario C. Comparison of bare-metal and sirolimus- or paclitaxel-eluting stents for aorto-ostial coronary disease. Cardiology. 2008;111:270-6. ]. Some concerns have been raised particularly on the use of the CypherTM stent in lesions of the right coronary ostium due to some reports of stent fractures in this location [1212. Popma JJ, Tiroch K, Almonacid A, Cohen S, Kandzari DE, Leon MB. A qualitative and quantitative angiographic analysis of stent fracture late following sirolimus-eluting stent implantation. Am J Cardiol. 2009;103:923-9. , 1313. Ohgo T, Otsuka Y, Furuno T. Complete fracture and restenosis of sirolimus-eluting stent in ostial saphenous vein graft. Int J Cardiol. 2008;128:e89-90. , 1414. Kamura A, Kawasaki T, Koga N, Inoue T, Node K. Fracture of a sirolimus-eluting stent with migration. Int J Cardiol. 2008;130:e86-8. ]. This stent platform, however, is no longer commercially available.
Procedural considerations
a) Femoral vs. radial access: either one is suitable and depends upon personal experience and individual anatomical or procedural considerations such as a tortuous subclavian artery or the size of the chosen guiding catheter.
b) Guide catheter positioning in aorto-ostial lesions: the critical issues are:
(i) to avoid occlusion of flow due to catheter wedging in the stenosis,
(ii) to avoid vessel dissection due to active and passive intubation of the diseased ostium, and,
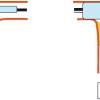
(iii) to be able to deliberately engage or disengage the guiding catheter for precise stent positioning, post-dilatation or further treatment of distal disease. Guide catheter disengagement may be achieved by anti-clockwise rotation of the catheter, by pulling back the guiding catheter and the wire, or, by putting forward pressure on the wire with only a slight pull on the guiding catheter. Re-engagement of the ostium can be achieved by clockwise rotation or by cautiously pulling on the guidewire keeping the guiding catheter in place ( Figure 1 ).
In challenging ostial disease, a ‘mother-and-child’ approach has been described using a 5 Fr catheter within a 8 Fr guiding catheter and two wires for additional stabilisation to achieve a stable position of the 8 Fr guiding in the coronary ostium [1515. Furuichi S, Sangiorgi GM, Colombo A. Coaxial double catheter technique followed by buddy wire placement for ostial lesion of right coronary artery with anterior take-off. Catheter Cardiovasc Interv. 2007;70:979-82. ].
c) Lesion preparation: aggressive debulking in ostial lesions has yielded conflicting mid-term results [1616. Airoldi F, Di Mario C, Stankovic G, Briguori C, Carlino M, Chieffo A, Liistro F, Montorfano M, Pagnotta P, Spanos V, Tavano D, Colombo A. Clinical and angiographic outcome of directional atherectomy followed by stent implantation in de novo lesions located at the ostium of the left anterior descending coronary artery. Heart. 2003;89:1050-4. , 1717. Kim YH, Hong MK, Lee SW, Lee CW, Han KH, Kim JJ, Park SW, Mintz GS, Park SJ. Randomized comparison of debulking followed by stenting versus stenting alone forostial left anterior descending artery stenosis: intravascular ultrasoundguidance. Am Heart J. 2004;148:663-9. ]. The use of cutting-balloons or rotational atherectomy, however, appears feasible for rigid and heavily calcified ostial lesions and may facilitate stent deployment and optimisation of stent apposition [1818. Motwani JG, Raymond RE, Franco I, Ellis SG, Whitlow PL. Effectiveness of rotational atherectomy of right coronary artery ostial stenosis. Am J Cardiol. 2000;85:563-7. , 1919. Nassar H, Gotsman I, Gerganski P, Moseri M, Lotan C, Gotsman M. Cutting balloon angioplasty and stent implantation for aorto-ostial lesions: clinicaloutcome and 1-year follow-up. Clin Cardiol. 2009;32:183-6. ].
d) Stent positioning in ostial lesions: full coverage of the ostium without unnecessary extension into the aorta or main vessel are key aims in stenting ostial lesions.
Difficulties with accurate positioning arise first and foremost from the choice of inappropriate angiographic views with foreshortening or overlap of the ostium. Additional and sometimes non-standard views are required to provide adequate visualisation ( Table 1 ). In aorto-ostial lesions the necessity for guide catheter disengagement frequently leads to poor opacification of the lesion. Stent deployment may be further complicated by excessive stent movement with respiration or systolic contraction.
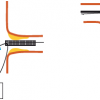
For exact positioning, it is critical to realise that the radio-opaque markers on the stent balloon usually do not mark the borders of the stent, but rather lie immediately proximal and distal from the stent ends. Thus, it is important to place the proximal marker immediately proximal to the ostium in order to fully cover the lesion ( Figure 2 ).
In ostial LAD disease, it has to be decided if precise positioning of the stent at the ostium should be attempted, or whether stenting back into the left main-stem is acceptable [2020. Capranzano P, Sanfilippo A, Tagliareni F, Capodanno D, Monaco S, SardellaG,Giordano A, Sangiorgi GM, Tamburino C. Long-term outcomes after drug-eluting stent for the treatment of ostial left anterior descending coronary artery lesions. Am Heart J. 2010;160:973-8. ].
e) Post-dilatation: After stent implantation, routine high-pressure post-dilatation with non-compliant balloons is highly recommended to assure optimal stent apposition. “Flaring” of the stent in aorto-ostial lesions by pulling back the stent balloon by half and re-inflating the balloon in the ostium may help to achieve full stent apposition due to the funnel shape of the aorto-coronary transition zone [2121. Kinoshita Y, Katoh O, Matsubara T, Ehara M, Nasu K, Habara M, Suzuki T. First clinical experience of “flower petal stenting”: a novel technique for the treatment of coronary bifurcation lesions. JACC Cardiovasc Interv. 2010;3:58-65.
Good technical paper on ostial bifurcation PCI.] ( Figure 3 ).
Technical considerations in ostial PCI
- Aorto-ostial lesions are often rigid and calcified
- Catheters with less support (e.g., Judkins shape) or short-tipped versions may be preferrable
- DES are preferred due to better clinical outcomes
- Guide catheter positioning in aorto-ostial lesions is critical to avoid occlusion of the vessel, vessel dissection, and for precise stent positioning
- Consider the use of debulking techniques for rigid and heavily calcified ostial lesions
- Achieve full stent coverage of the ostium without unnecessary extension into the aorta or main vessel
- Choose appropriate angiographic views without foreshortening or overlap of the ostium
- Post-dilatation: after stent implantation routine high-pressure post-dilatation with non-compliant balloons is highly recommended
Special techniques
a) Draw-back stent deployment technique: the draw-back technique is used preferably for non aorto-ostial lesions with a bifurcation angle of >75° [2222. Schwartz L, Morsi A. The draw-back stent deployment technique: a strategy for the treatment of coronary branch ostial lesions. J Invasive Cardiol. 2002; 14:66-71.
Good technical paper illustrating the draw-back technique.]. It requires the placement of a second wire in the non-target vessel ( Figure 4 ). Thereafter, the stent is advanced beyond the lesion in the target vessel. A slightly undersized compliant balloon is advanced over-the-wire in the non-target vessel opposite the target ostium. After low pressure inflation of the balloon with 6-8 atm the stent is pulled back until an indentation is observed on the balloon and the stent is then inflated. Both balloons are deflated and removed.
b) The “tail-wire” technique: this technique has been developed by Szabo et al, for aorto-ostial lesions but may also be used for non-aorto-ostial lesions. It utilises a second angioplasty wire positioned in the aorta to anchor the stent at the ostial location [2323. Szabo S, Abramowitz B, Vaitkus PT. New Technique of Aorto-Ostial Stent Placement. Am J Cardiol. 2005;96: 212H.
Original description of the Szabo technique, unfortunately only in abstract form., 2424. Applegate RJ, Davis JM, Leonard JC. Treatment of ostial lesions using the Szabo technique: a case series. Catheter Cardiovasc Interv. 2008;72:823-8. , 2525. Kern MJ, Ouellette D, Frianeza T. A new technique to anchor stents for exact placement in ostialstenoses: the stent tail wire or Szabo technique. Catheter Cardiovasc Interv. 2006; 68:901-6.
Excellent description of the Szabo technique.].
After placing one wire in the target vessel and one wire either in the aorta or in the non-target vessel, the stent is loaded onto the target vessel wire and the proximal end of the aortic or non-target vessel wire is threaded through the most proximal strut of the stent. The threading can be facilitated by partly applying pressure to the stent balloon until the proximal end flares which requires manual re-crimping of the stent ( Figure 5 ). The stent catheter is then advanced into the ostial lesion until the “tail-wire” stops its forward motion whereupon the stent should be deployed precisely at the ostium ( Figure 6 ). However, recent bench testing and in-vivo IVUS examination observed, despite a seemingly excellent immediate result, a significant and asymmetric stent protrusion into the main branch, with the last cell of the stent undergoing significant deformation [2626. Vaquerizo B, Serra A, Ormiston J, Miranda-Guardiola F, Webber B, Fantuzzi A, Delgado G, Brugera J. Bench top evaluation and clinical experience with the szabo technique: New Questions for a Complex Lesion. Catheter Cardiovasc Interv. 2012;79:378-89.
Small but excellent and critical in-vitro and in-vivo study on the correctness of ostial stent placement with the Szabo technique.]. Thus, the true benefit of this technique remains to be determined.
Complications
a) Typical complications in ostial lesions are dissections of the vessel by aggressive or unintentional guide catheter manipulation. These may be avoided by careful catheter manipulation, the use of less aggressive catheters, or guidewire preloading for rapid stabilisation of the catheter in the ostium.
b) Dissection can also occur after stent deployment at the edges of the stent. This may be avoided by careful stent implantation and successive post-dilatation. In this context it is important to realise that manufacturers often mount the same stent on different balloon sizes (individual information required for each stent type), thus, the initial intentional use of a slightly smaller stent system with careful post-dilatation up to the desired size is feasible.
c) The loss of guide catheter position can be avoided by using a buddy wire for additional support.
d) Inadequate stent expansion in rigid and heavily calcified ostial disease can be avoided by appropriate lesion preparation including debulking techniques.
e) Excessive protrusion of the stent into the aorta or the respective main vessel can be avoided by direct, unforeshortened visualisation with no vessel overlap and by the use of specific stent placement techniques such as the “pullback” and maybe the “tail-wire” technique.
f) Incomplete coverage of the ostium by placing the stent too distally into the ostium which can be avoided as above by optimal visualisation of the ostium and possibly by the use of specific stent placement techniques.
Conclusions
The most important factor in achieving an optimal result when treating ostial lesions is, first and foremost, a thorough assessment in order to have a clear idea of its nature. In addition to precise angiographic imaging for optimal strategic planning, this requires the evaluation of the haemodynamic relevance, as well as a description of the complexity, of the lesion. The anticipation of, and ability to handle, specific complications are crucial to immediate interventional success. Dissections, and incomplete stent expansions are frequently seen and can be avoided by adequate lesion preparation. Lesions should be stented with drug-eluting stent platforms whenever possible, and, precise handling of the material with full coverage of the ostium is essential to achieve the lowest possible restenosis rates, which are still significantly higher than in non-ostial lesions.
Personal perspective - Christoph K. Naber
We are currently able to handle ostial stenoses reasonably well. This is true for aorto-ostial stenoses including the left main stem, as well as for non-aorto-ostial stenoses. Personally, I would like to stress four points:
a) The indication for PCI should be stringent and based on either prognosis or symptoms;
b) Lesion assessment should be precise and allow us to plan the PCI strategy in advance;
c) Even more so than in non-ostial lesions, an optimal technical result is key to immediate and long-term success.
d) Optimal visualization of the ostium without overlap or foreshortening is the most important factor to achieve this goal.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
What about 1-FLASH™ Ostial System 2-Ostial Pro stent positioning system?
In Non aorto-ostial lesions where the target daughter vessel has a distal angle different from 90, one needs to balance between protusion of stent in the main vessel versus a small triangular area of uncovered endothelium by the stent; draw-back stent deployment tactic may not be possible always as in ostial LCx position. Also it may not be always be possible to estimate stent length shortening when inflated at high pressures. Dr Kanha Vijay Singru
I find this quite useful and practical ,, I've a patient with ostial RCA lesion ,, so i checked here to remind my self with the steps ,, very useful really ,,remembered ostial lesions are no so common in daily cath lab work, this what we need , a text that guide your daily practice
How come no mention of the Ostial Pro stent positioning system...?
Another technique it would be the sepal wire for aorto-ostial stenosis