



Case presentation
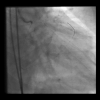
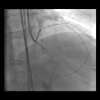
The case was a proximal LAD CTO, with an ambiguous proximal cap, >40mm length, small distal vessel, which was visualized via Left-to-Left epicardial collaterals from the proximal diagonal branch, of which a proximal tight disease was treated by DES deployment for ACS ( Video 1). PCI attempt was made by bilateral approach for remaining angina, with unsuccessful wire crossing over the proximal cap. The second attempt was made by bifemoral 7F access, using the 45cm long sheathes. RCA injection demonstrated a trace of collateral connection immediately over the crux of the RCA to a LAD across a septum ( Video 2), which was successfully crossed by a Suoh 03 wire over a Turnpike LP microcatheter (Teleflex, USA) ( Figure 1), and an Ultimatebros 3g (Asahi Intecc, Japan) reached up to the proximal cap at the side of the diagonal stent ( Figure 2).
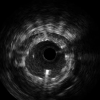
First, IVUS pullback from the diagonal branch could not spot the retrograde wire partially due to the circumferential overshadowing of the high echogenic stent struts ( Video 3). So, a 3.0 mm balloon was advanced over the stented segment ( Video 4), and briefly ballooning served as a target and support of a retrograde puncturing over rotational fluoroscopic imaging ( Video 5).
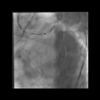
After the crossing failure of Gaia 3, Confianza pro12, and Hornet 14, an Astato 20 (Asahi Intecc, Japan) succeeded in crossing through the stent struts, confirmed by IVUS ( Video 6), followed by a Turnpike LP crossing. After guidewire externalization by an RG3 330cm, the proximal cap was dilated first by a new 2.0 mm balloon ( Figure 3), and placement of a workforce wire into a distal LAD by a dual lumen catheter made the remaining ballooning and stenting possible with a quite favorable outcome ( Video 7).
Although it was a stiff Guidewire to penetrate through a previously deployed stent, effect of bi-femoral long sheaths, support of a microcatheter closer to a wire tip, balloon inflation inside the stent, and rotational fluoroscopy to keep a wire tip as much as perpendicular to a stent strut, could synergistically provide a final positive outcome.

{kind=link}
{kind=link}
{kind=link}
{kind=link}