



Case presentation
The non-dominant LCX CTO, with a clearly defined proximal cap, >30mm length, distal cap at a bifurcation, and ipsilateral epicardial-collateral from a diagonal branch (J-CTO score 1), was approached by a single 8F AL 1.0SH Guide catheter ( Video 1). Antegrade wiring started with a Fielder XT-R and Gaia Next 1 (Asahi Intecc, Aichi, Japan), with probable subintimal wiring to the main LCX branch ( Video 2).
ADR was attempted by a replaced Guidewire of Miracle 12g and a Stingray LP (Boston Scientific, USA), by which Double-blind stick and swap with a Bobsled technique carried out by a Gaia Next 2 ( Video 3) (Asahi Intecc, Aichi, Japan), but the wire resulted in a subintimal space ( Video 4).
The contrast-guided collateral crossing was then undertaken from a LAD Diagonal branch, leaving the first antegrade wire kept in place as a marker ( Video 5). A Souh 03 wire crossed the epicardial collateral ( Video 6) and reached the distal bifurcation ( Figure 1).
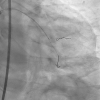
When a Finecross microcatheter encountered some resistance close to the curve tip, the wire lunged in a straight direction ( Figure 2). Immediate contrast injection confirmed epicardial collateral rupture ( Video 7), followed by 0.014 in compatible coil delivery (C-stopper coil 2.0mmx15mm, Piolax Medical, Japan) ( Video 8).
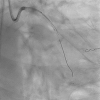
Serial angiography reconfirmed hemostasis, and retrograde access was then, abandoned. Antegrade Guidewire exchanged to a workforce wire of Sion, IVUS (Alta view, Terumo, Japan) pullback was performed ( Figure 3), which demonstrated a subintimal progression of a wire with a large hematoma and proximal true lumen ( Video 9).
Re-puncturing attempted for a Gaia Next 3 to get to the intimal plaque ( Figure 4), which succeeded and was confirmed by IVUS ( Video 10).
A Sionblue wire replaced the Gaia Next in the distal LCX over a microcatheter advancement by trapping ( Figure 5), and the second wire of Sion onto the large OM branch after IVUS confirmed the uninjured anatomy of the bifurcation ( Video 11). A 2.0 mm balloon dilation in the distal LCX and a 2.5 mm balloon dilation in the OM branch, respectively, enabled a long DES deployment over the bifurcation toward the OM, and post NC balloon dilation achieved an excellent outcome ( Video 12).
The case demonstrates the importance of intra-procedural changes once fallen into a failure or stalemate mode, without leaving a potential complication.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}