



Case presentation
The case is an ostial RCA CTO, characterized by a blunt calcified proximal cap, >90 mm length, poor distal landing near the crux of RCA, bending inside, prior failed attempt, and interventional collaterals ( Video 1, 2). A retrograde approach was deemed mandatory and started by a selective injection over a major septal branch, which depicted a continuous, but tiny rudimental collateral in the lower septum ( Video 3).
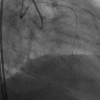
The collateral crossing was obtained by a Suoh 03 ( Figure 1), which navigated a Corsair pro to the PDA, through which a pure contrast injection described detail anatomy (a retrograde filling before an RCA bifurcation, which is a favorable sign for wiring ( Video 4).
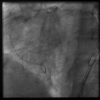
CTO crossing was partially navigated by peri-vascular radiopacity ( Video 4). A Gaia 3 reached a middle segment ( Figure 2), where a strong resistance was met and necessitated a Confianza Pro 12 to cross the remaining occlusion ( Figure 3).
The proximity of the retrograde wire allowed the use of stiffer wire of antegrade Confianza Pro 12, which stayed distant in RAO cranial projection ( Figure 4).After 1.5 mm balloon dilation, IVUS demonstrated an IVUS probe (a white arrow in Figure 5) in the true lumen. A retrograde wire in a subintimal space (a yellow arrow in Figure 5).
Therefore, drive intimal wiring deeper (When antegrade wiring, deeper means more distal to re-enter, when retrograde, deeper means more proximal to re-enter) is a key for resolving separation of 2 gears in reverse CART. Antegrade wiring of Astato 20 provided proximity with a retrograde wire in the middle segment ( Figure 6), where a 1.50 mm and 2.0mm ballooning was conducted for reverse CART ( Figure 7).
A retrograde wire pulled back beyond the ballooning site to re-enter the same antegrade wiring space (via reverse CART), which succeeded. ( Figure 8). After successful wire externalization by an RG3 330cm and 1.5 mm balloon dilation, IVUS revealed mostly an intimal wire tracking with some hematoma ( Figure 9, Video 5).
Full patency was restored after meticulous NC balloon dilation throughout the CTO and stenting starting partially over a distal bifurcation back to an ostium ( Figure 10, Video 6).
The case illustrates the importance of IVUS application when dealing with a problematic reverse CART (RDR): when an intimal wire advances deeper, which facilitates re-entry by a reverse CART.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}