



Case presentation
PCI re-attempt was made for a proximal RCA CTO characterized by a blunt proximal cap, long occlusion, heavy calcification, poor distal landing before a distal bifurcation, and probable interventional collateral through LAD septal (J-CTO score of 4, Video 1). The CTO was approached by the bifemoral 7F system, which visualized a poorly defined distal target ( Video 2).
The primary retrograde approach was adopted as an initial strategy, starting a collateral injection of LAD in RAO projection ( Video 3). A Suoh 03 expeditiously crossed a major septal to a PDA over a Turnpike LP microcatheter (Teleflex, USA) ( Video 4). An escalation of a wire from Ultimatebros 3g to Gaia Next 3 enabled the retrograde system to reach more advanced in the calcified CTO.
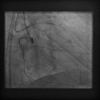
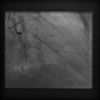
An antegrade Gaia Next 3 also advanced an overlapping position within the occlusion in the LAO projection ( Figure 1). However, the inability of 1.50mm ballooning beyond the bend failed a retrograde wire to implement reverse CART in RAO projection ( Figure 2).
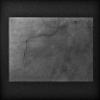
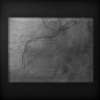
The second wire of Confianza Pro 12 with a small (< 1mm), sharp bend (>60°) over a Sasuke (a dual lumen microcatheter) was targeting more closer crossing over a retrograde wire ( Figure 3), which achieved a little overlaying in the middle segment. A 2.0 mm balloon was dilated over a merging point of both guidewires to implement reverse CART ( Figure 4).
Further balloon dilation back to the proximal accompanied a retrograde wire in overlaying position ( Figure 5), which entered a guide extension through an antegrade guide ( Figure 6).
Following a Turnpike LP entered an extension, a guidewire exchanged to an RG3 for externalization ( Figure 7), over which incremental balloon dilations were carried out from 1.50mm to 2,5mm, and long DESs were safely delivered ( Figure 8) and deployed ( Figure 9). An excellent result was achieved ( Video 5).
The case illustrates creating a merger point by a second antegrade wire has resolved difficulty in reverse CART for recanalizing heavily calcified bending CTO.






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}