



Case presentation
The case is a long LAD CTO, consisting of a tapering proximal cap (including InStent Restenosis=ISR), long occlusion, poor distal landing, and no interventional collaterals ( Video 1, 2). LVEF is within normal limits with modest exertional angina. PCI started with 7F systems for Left and Right, and Fielder XT-R (Asahi Intecc, Japan) ( Video 3) and Gaia Next1(Asahi Intecc, Japan) reached out close to the distal cap, without clear visualization from any collaterals ( Video 4).
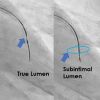
Guidewire had exchanged to a MiracleNeo3g (Asahi Intecc, Japan), over which a 1.5 mm balloon inflation was performed, followed by an IVUS exam (Terumo Alta-view, Tokyo Japan, a mechanical scan of 60 MHz) ( Figure 1). Pull back IVUS revealed cross-sections of subintimal space (a yellow arrow indicated an intimal plaque), transitioning from subintimal to the true lumen ( Video 5).
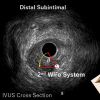
When 7 F Guides are applied, low profile IVUS of mechanical scan such as Terumo, Boston can accommodate a second wire and microcatheter system inside together. After the system reached the tip close to the IVUS ( Figure 2), identify the broadest view between an IVUS probe and a second Wire-micro system by rotating the Image Intensifier along a longitudinal axis of the target segment ( Video 6). In this case, the left lateral projection separated most for the two gears.
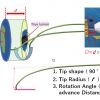
When a second puncture wire enters in a tip toward the pericardium in Figure 11, one can orient the Left lateral view projects from 8 o'clock on the IVUS cross-section ( Figure 4). So maximum radius to puncture has to cover the distance r (usually 2-2.5mm, so addition curve required in case of Gaia Next 3), and angle over which the wire covers has to be θ from proximal true ( Figure 4) to the distal intimal plaque ( Figure 3). Therefore, a wire has to deflect counterclockwise rotation while advancing over the distance of d, which is usually given by pullback IVUS measurements. A stiff wire of Confienza Pro 12g (Asahi Intecc, Japan), Hornet 14 (Boston Scientific, USA), GaiaNext2, 3 (Asahi Intecc, Japan) is applicable for this puncture.
Wire travels a distance D, which is about x1.2 longer distance in mm, considering a wire crosses d mm ( Figure 5) and deflects at the intimal cap to penetrate ( Figure 6). When the IVUS interferes with a second wire deflection, IVUS pulls back a little would be of help ( Figure 7). When the wire hits the bull's eye of the intimal plaque, an operator may feel a subtle resistance at the tip, and IVUS will confirm the position ( Video 7). When the tip is in the intima, a microcatheter had better advance to the wire tip (but not beyond) and swap the wire to a middleweight wire (an Ultimatebros 3g (Asahi Intecc, Japan), with an original pre-shaped tip) ( Figure 8). Careful probing (or drilling) navigates a wire into a distal true lumen. When doubt of wire position remained in this case, we use a Suoh o3 to track a distal vessel after the advancement of the microcatheter ( Video 8). After wire position was confirmed both in angiography and IVUS ( Video 9 and 10), a 2.0 mm balloon dilated softly to the tip. A 2.5 mm Drug-Eluting Stent (DES) deployment with partially overlapping prior stent and DEB (Drug-Eluting balloon) dilation further down the vessel achieved a good TIMI 3 flow down to the apical segment ( Video 11).
This illustrates a different approach for IVUS navigated intimal puncture, explained in the main text. Both emphasize practical solution in complex, difficult situation of antegrade wiring.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}