Summary
Cardiac catheterisation in children and adults with congenital heart disease is of increasing importance due to the rising number of newborns with congenital heart defects reaching adulthood. In addition to diagnostic catheterisation, interventional catheterisation is an essential tool for treatment of sequelae following corrective or palliative treatment of complex congenital heart disease. Ever since the first case of neonatal transcatheter intervention by Rashkind in 1967 [11. Watson H, Rashkind WJ. Creation of atrial septal defects by balloon catheter in babies with transposition of the great arteries. Lancet. 1967;1:403-5. ], numerous percutaneous interventions have been introduced to the field and have enriched our armamentarium of treatment options for these patients.
The complexity and heterogeneity of children and adults with grown-up congenital heart disease require an individualised plan and approach for catheterisation.
Introduction
In the past, diagnostic cardiac catheterisation and angiography were the gold standard for imaging and haemodynamic assessment in patients with congenital heart disease. With the evolution of non-invasive imaging techniques, such as echocardiography and magnetic resonance imaging, many congenital defects can now be diagnosed and treated solely on the basis of these methods. However, in the presence of inconclusive or contradictory non-invasive imaging data or unexplained unfavourable clinical developments, diagnostic catheterisation is still mandatory to help reach a definitive diagnosis.
In particular, more complex lesions demand thorough and precise diagnostic catheterisation to obtain detailed anatomic and haemodynamic information. A sound knowledge and understanding of these is paramount for the success of contemporary advanced surgical, percutaneous or hybrid treatments.
A further indication for cardiac catheterisation is the fast developing field of therapeutic catheter interventions.
Although there are many standardised catheterisation procedures for specific lesions and situations, there is no general standardised catheter approach to the vast variety of frequently complex congenital cardiovascular malformations. Detailed knowledge of the individual patient’s history, clinical data and non-invasively acquired information are crucial for planning and performing cardiac catheterisations in patients with congenital heart disease or its sequelae following corrective or palliative treatment. Anomalous anatomical courses of vessels may require alternative means of vascular access. Historical surgical procedures (e.g., the Waterston and classic Blalock-Taussig-shunt and their distinct anatomical patterns and haemodynamic effects) have to be understood and sometimes institutional or individual operator modifications (with reference to the original surgical handwritten record) must be considered. Specific problems and complications associated with certain types of treatment (e.g., baffle stenosis following atrial repair for transposition of the great arteries or venovenous collaterals developing after cavopulmonary anastomosis) have to be anticipated, identified and circumvented [22. Mullins CE. Cardiac catheterisation in congenital heart disease: pediatric and adult. Blackwell Futura; 2006.
One of the best books on catheterisation in congenital heart disease.].
This chapter will cover some specific aspects of cardiac catheterisation in children and adults with grown-up congenital heart disease, focusing on issues relevant to the cardiologist dealing with adult patients. Whereas specific congenital interventions such as closure of shunts, valvuloplasty, percutaneous valves and coarctation are covered in individual chapters, here we will concentrate mainly on diagnostics. Within the text, the terms newborn and neonate are interchangeable and refer to the first 28 days of post-natal life, whereas infant refers to the first year of life, and child the period from infancy to adulthood.
Indications for catheterisation in children and adults with congenital heart disease
- Insufficient or conflicting non-invasive data
- Unexpected and/or unexplained unfavourable clinical course
- Intended interventional treatment
Contraindications for catheterisation in children and adults with congenital heart diseaseAbsolute contraindications:
- Sufficient non-invasive information already available
- No previous non-invasive assessment
- Lack of potential therapeutic/management consequences as a result of catheterisation
Relative contraindications:
- Uncontrolled coagulation disorder
- Sepsis or septic shock
- Severe hemodynamic compromise
Risks of catheterisation in children and adults with congenital heart disease
- Bleeding
- Thrombosis
- Trauma to vessels and cardiac structures
- Cardiac tamponade
- Arrhythmia
- Pulmonary or systemic embolism
- Allergic reactions
- Consequences of radiation exposure (children, young adults and females being especially prone to biological effects)
Principles of catheterisation in children and adults with congenital heart disease
- Meticulous indiviudual planning
- Selection of the least traumatic and most effective vascular access
- Maximal reduction of radiation exposure
- Combination with non-invasive imaging
- Combination of diagnostic and therapeutic procedures within one session
General considerations
THE SET-UP
There should be a designated catheterisation laboratory for children and adults with congenital heart disease [33. Brzezinska-Rajszys G, Carminati M, Qureshi SA. The ideal configuration of the modern theatre for paediatric cardiac catheterisation: Recommendations of the Association for European Paediatric Cardiology. Cardiol Young. 2003;13:582-4. ]. If interventional procedures, especially device implantations, are performed, the laboratory should implement features and policies common to operating theatres and conventional cardiac catheterisation laboratories. Bi-plane fluoroscopy (with two movable C-arms) with flat panel detector technology are recommended in order to achieve low radiation doses, high resolution, high frame rate and digital image storage. Additional monitors for the display of still frames as roadmaps are desirable. Some contemporary laboratories also have integrated monitors linked to an echo machine for the simultaneous display of transthoracic/transesophageal echocardiographic and fluoroscopic imaging.
Monitoring such as ECG, invasive pressure recordings and haemodynamic analysis designed for use in congenital cardiac malformations is mandatory.
The catheterisation laboratory should be equipped with power injectors for contrast media, analysers for blood oxygen saturations, blood gas analysis, activated clotting time and emergency equipment for resuscitation (defibrillator, external pacemaker, anaesthetic equipment), with the latter in all sizes/specifications required for patients from newborns to adults.
A large stock of needles, short and long introducer sheaths, guidewires, diagnostic and therapeutic catheters, implants (i.e., stents, occluders, coils) and hardware required for management of complications is needed to cover both all patient sizes and all possible diagnostic and therapeutic procedures.
PREPARATION
In order to understand the patient’s haemodynamic status and ask the relevant questions that can be answered by cardiac catheterisation it is mandatory to study the sometimes very complex patient history, including all previous cardiovascular findings, catheterisation procedures and surgical and/or percutaneous interventions as well as clinical findings, non-invasive images and lab values. There should be an individual plan for each scheduled catheterisation. In neonates, infants and small children one unit of erythrocytes should be prepared for potential transfusion.
SEDATION AND ANAESTHESIA
In children, diagnostic catheterisation is usually performed under sedation or general anaesthesia or a combination, according to local practice. For example some centres perform analgosedation with ketamine and midazolam.
In adults, local anaesthesia is usually sufficient. However, sedation or general anaesthesia is used in complex interventions and procedures requiring simultaneous imaging with transesophageal echocardiography. For the latter, sedation with propofol is favoured by many practitioners.
ANTIBIOTIC PROPHYLAXIS
Routine antibiotic prophylaxis is not recommended for diagnostic catheterisation of children and adults with congenital heart disease. However, it might be considered in more prolonged and complex procedures. Despite the lack of data supporting its use, most centres prefer a periprocedural antibiotic when permanent devices are implanted (such as a stent, occluder, plug, coil, or valve). There is no need for antibiotics in other interventional procedures. The antibiotics most frequently used are cefazolin and cefuroxime. In patients allergic to cephalosporins, vancomycin or clindamycin may be used.
HEPARINISATION
In children a dose of 100 IU/kg of heparin should be administered after vascular access is obtained. In prolonged procedures, half the dose is repeated every two hours. Activated clotting time (ACT) can readily be measured to monitor heparin’s anticoagulant effect. For some interventions an activated clotting time of 200 seconds or more is recommended. If either transseptal puncture or endomyocardial biopsy is planned, it is advisable to give heparin only after this procedure has been performed successfully and pericardial effusion has been ruled out.
Vascular access
Choice of vascular access depends on the planned diagnostics and intervention and the patient’s anatomy including congenital or acquired vessel anomalies, obstructions and occlusions.
Percutaneous puncture of femoral arterial and venous vessels is the standard access for cardiac catheterisation in children and adults. The technique is not very different in children from the one used in adults, except that in infants and young children the puncture site is chosen more distally, and the angulation of the needle more horizontal than in adults. Smaller sheaths (3 and 4 French) with thinner guidewires (0.018” and 0.021”) are used.
JUGULAR/CAROTID
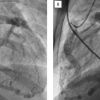
Percutaneous puncture of the jugular vein is commonly performed in patients with congenital heart disease. It is an alternative to femoral venous access if the femoral, iliac or inferior caval veins are occluded. It is the access of choice to reach the pulmonary arteries in patients with an upper cavopulmonary anastomosis (Glenn) ( Figure 1 ), and to implant occluders in mid-muscular and apical ventricular septal defects. The right jugular vein is often used to perform endomyocardial biopsy.
The carotid artery is rarely used for catheterisation purposes. Some practitioners have found it a useful access point for aortic balloon valvuloplasty in neonates and infants.
SUBCLAVIAN/AXILLARY/BRACHIAL/RADIAL
The subclavian vein is a routine access for indwelling central venous catheters and pacemaker leads. It can also be used as an alternative access for diagnostic and interventional catheterisation but percutaneous puncture carries a higher risk of bleeding and pneumothorax as compared to the jugular approach. Sometimes, the axillary vein is also used as an access. Brachial veins may also be accessed but they have no anatomically defined course. Their tortuousity may be challenging to overcome even with thinner catheters and subsequent intracardiac steerability may be compromised. Large sheaths or catheters should not be inserted into brachial veins. The veins of the hand and forearm are not suitable for cardiac catheterisation access. By contrast, radial arterial access is often used nowadays in coronary angiography and interventions and it may be used for diagnostic procedures or as a second arterial access in complex interventional procedures in older children, adolescents and adults ( Illustrative case). Brachial and axillary arteries are alternative access routes for arterial catheterisation requiring larger sheaths, while the subclavian artery should not be approached.
TRANSHEPATIC
In special situations transhepatic access may also be attempted by percutaneous puncture of the hepatic veins through the liver. Such circumstances might include occluded femoral, subclavian and jugular veins, anticipated challenging transseptal punctures or planned closure of atrial septal defects in patients with occluded femoral veins, an interrupted inferior caval vein or an azygous continuation [44. Shim D, Lloyd TR, Cho KJ, Moorehead CP, Beekman RH, 3rd. Transhepatic cardiac catheterization in children. Evaluation of efficacy and safety. Circulation. 1995;92:1526-30. ].
UMBILICAL
Umbilical access is possible only in newborns, most often in the first three days after birth, sometimes up until the end of the first week of life. The access route is most often used to perform balloon atrioseptostomy (Rashkind manoeuvre) in newborns with transposition of the great arteries and poor mixture or other cyanotic lesions with restrictive interatrial communication [55. Zeevi B, Perry SB, Keane JF, Mandell VS, Lock JE. Interventional cardiac procedures in neonates and infants: state of the art. Clin Perinatol. 1988;15:633-58.
This work gives insights into interventions in neonates and infants.]. Neither umbilical venous access (which directs the catheter towards the roof of the left atrium) nor the umbilical arterial access (which forms a U-turn from the retrograde “descending” umbilical artery via the “ascending” internal iliac artery to the descending aorta) is well-suited for extensive diagnostic or interventional catheterisation.
Haemodynamic assessment
(  View chapter and View chapter )
View chapter and View chapter )
Details of right and left heart catheterisation and haemodynamic measurements are subjects of a different chapter in this textbook. In general, assessment of haemodynamics in children and adults with grown-up congenital heart disease does not differ fundamentally from patients with acquired heart disease. However, assessment of pullback or simultaneous measured pressure gradients is of particular importance in these patients, due to various obstructions at multiple sites (e.g., stenosis of pulmonary arteries) or obstruction of venous pathways (e.g., atrial baffles after atrial switch procedure). Therefore, the use of the Multi-Track™ catheter (NuMed Inc., Hopkinton, NY, USA) is considered helpful by many practitioners, since it allows for accurate assessment and manipulation supported at the same time by the guidewire.
Angiography
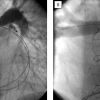
Again, the commonly used equipment, settings and techniques of angiography are accordingly applied to children and adults with congenital heart disease. Biplane fluoroscopy should be standard. In addition to conventional angiographic views, specific projections and angulations are useful for visualisation of congenital defects. The long axial oblique view is obtained in a 60 to 70 degree left anterior oblique with a 20 to 30 degree cranial angulation. In left ventriculography, this view allows for demonstration of mid, apical and perimembranous ventricular septal defect, left ventricle to right atrium (Gerbode) shunts, the subaortic area and the aortic arch ( Figure 2 ). The right anterior oblique orthogonal view is useful for assessment of anterior and subpulmonary septal defects and of the right ventricular outflow tract in tetralogy of Fallot. The hepatoclavicular view or four-chamber view (~40 degree left anterior oblique with ~40 degree cranial angulation) is best suited for assessment of the atrioventricular canal/area. LAO and frontal views with cranial angulations usually provide the best information on the pulmonary bifurcation.
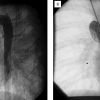
Nevertheless, conventional frontal and lateral views are of importance for visualisation of certain anatomic areas (e.g., systemic and pulmonary venous drainage, pulmonary stenosis, right ventriculography, anatomy of coronary arteries) ( Figure 3 ) and in all cases of unknown and complex anatomy, as an initial orientation.
Assessment of cardiac shunts
Intra or extra-cardiac shunts are common in patients with congenital heart disease. Both intra and extra-cardiac defects can lead to either left-to-right, right-to-left or bidirectional shunting. Whereas shunts can be detected using echocardiography, invasive angiography or three-dimensional imaging techniques such as magnetic resonance imaging, this section will focus on the detection and quantification of cardiac shunts using oxygen content and saturations [66. Wilkinson JL. Haemodynamic calculations in the catheter laboratory. Heart. 2001;85:113-20.
Standard work on oximetric detection of intracardiac left-to-right shunt.].
LEFT-TO-RIGHT SHUNTS
Left-to-right shunting can occur due to various intra and extra-cardiac defects such as atrial and ventricular septal defects, an aorto-pulmonary window or a patent ductus arteriosus. Whereas an isolated atrial septal defect in children usually causes left-to-right shunting, shunt directions are not defined by the diagnosis per se but instead depend on the instantaneous pressure gradients across the defect. This also means that secondary pulmonary hypertension, for example due to a large ventricular defect, will lead to a change in shunting direction from left-to-right to right-to-left as a result of an increase in pulmonary vascular resistance over time. Intra-cardiac left-to-right shunting will cause an increase in oxygen saturations in the right heart and pulmonary arteries. To detect and quantify left-to-right shunting, blood samples have to be taken from all right-sided compartments. Left-to-right shunting can be considered to be present if saturations exceed the normal variation for the individual compartment or increase downstream from vena cava to pulmonary artery. Thus, a rise in right atrial saturations greater than 5% to 6% compared to saturations in the superior vena cava is suggestive of atrial left-to-right shunting [77. Freed MD, Miettinen OS, Nadas AS. Oximetric detection of intracardiac left-to-right shunts. Br Heart J. 1979;42:690-4. , 88. Esmaeili A, Hohn R, Koch A, Vogl TJ, Hofstetter R, Abolmaali N. Assessment of shunt volumes in children with ventricular septal defects: comparative quantification of MR flow measurements and invasive oximetry. Clin Res Cardiol. 2006;95:523-30. ].
RIGHT-TO-LEFT SHUNTS
In the presence of intra-cardiac right-to-left shunting, blood flows from the right heart to the left heart. This causes a decrease in left-sided saturations. Therefore in contrast, to left-to-right shunting, any evidence for decreased oxygen saturations in the left heart is diagnostic for right-to-left shunting. In clinical practice, an arterial saturation < 95% in a left-sided compartment has to be considered the result of right-to-left shunting until proven otherwise.
QUANTIFICATION OF SHUNTS
Assessment of oxygen content or saturations of the blood in the various chambers and great vessels allows for the detection and quantification of shunts as discussed above. By using oxygen content (O2 con) and oxygen consumption (VO2), pulmonary blood flow and systemic blood flow can be calculated as follows:
Pulmonary blood flow = VO2/(PV O2 con - PA O2 con)
Systemic blood flow = VO2/ (SA O2 con - MV O2 con)
Where PV is pulmonary vein, PA is pulmonary artery, SA is systemic artery, and MV is mixed systemic venous, consisting of superior and inferior venal caval blood and coronary venous blood.
Due to variable mixing of blood in the right atrium, mixed systemic venous saturations are derived from pulmonary artery saturations, in the absence of cardiac shunts.
In the presence of left-to-right shunts, mixed venous saturations should be obtained proximal to the level of shunting. Similarly, in the presence of right-to-left shunting, the oxygen content should be measured proximal to the site of shunting for calculation of pulmonary blood flow.
To define the level of shunting, an oximetry run should be performed in a stepwise fashion. Blood samples should be taken from: left and right pulmonary artery, main pulmonary artery, right ventricular outflow tract, right ventricle, right atrium, proximal and distal (just below the entry of the innominate vein) vena cava superior, proximal and distal (between hepatic and renal veins) vena cava inferior, left ventricle, and aorta. In some cases, blood samples from each pulmonary vein should be taken as well (see below). A shunt can be considered to be located between the levels of significant (5% to 7%) differences in saturations.
The shunt can be quantified according to the Fick principle. As outlined above, a left-to-right shunt increases pulmonary blood flow (QP) compared with systemic blood flow (QS) and the shunt can be calculated as follows:
QL-R = QP - QS
According to the equations outlined above, the pulmonary to systemic flow ratio (QP/QS) can be calculated according to the following equation:
QP/QS = (SA O2 – MV O2) / (PV O2 – PA O2)
In acyanotic patients, PV O2 is generally considered to be equal to SA O2. However, in cases of decreased systemic saturations, PV O2 should be determined by obtaining blood samples in the left atrium and each individual pulmonary vein. Furthermore, in children, superior vena caval oxygen saturations are taken as the MV O2 [99. Lock JE. Cardiac Catheterization. In: Keane JF, Lock JE, Fyler DC, Nadas AS, eds. Nadas’ Pediatric Cardiology. 2nd ed. Philadelphia: Saunders Elsevier; 2006:1 online resource.
An excellent chapter on cardiac catheterisation in congenital heart disease.]. Alternatively, MV O2 can be estimated using the more complex equation:
MV O2 = ((superior vena caval O2 x 3) + inferior vena caval O2) / 4 [1010. Frederick A, Heupler J. The Sience of Hemodynamic Measurements. In: Griffin BP, Rimmerman CM, Topol EJ, eds. The Cleveland Clinic cardiology board review. Philadelphia: Lippincott Williams & Wilkins. 2007. ].
Differentiation between shunting and lung disease
Left-sided desaturations can also be due to significant lung disease. If there is any suspicion of lung disease, the oxygen content in the left atrium and in each individual pulmonary vein should be obtained. If saturations in the pulmonary veins are low, lung disease is likely. For further differentiation, 100% oxygen can be administered, which should lead to a marked improvement in arterial oxygen saturations in the presence of lung disease, whereas significant intra-cardiac shunting should be only mildly affected. Furthermore, if left-sided desaturation is due to intra-pulmonary shunts such as are seen in arterio-venous malformation, arterial saturations will increase only modestly after administration of 100% oxygen.
Limitations of shunt quantification
In certain lesions, it is impossible to obtain accurate mixed saturations for shunt calculations. For example, a patent ductus arteriosus usually results in higher saturations in the left pulmonary artery as compared to the right pulmonary artery, since blood flow from the aorta to the left pulmonary artery will increase relative to the right pulmonary artery. Moreover, using an average of saturations in the left and right pulmonary arteries assumes an equal blood supply to the left and right lung. Similarly, in patients with anomalous pulmonary venous return, it is not possible to obtain mixed venous saturations. Finally, in atrial septal defects, obtaining a reliable mixed venous saturation is doubtful. In all these conditions, flow calculations by magnetic resonance imaging represent the superior technique.
In patients with multiple shunts, shunt calculations can be challenging. The different degree of shunting at each individual anatomical level (e.g., on atrial level as in atrial septal defects and on ventricular levels as in ventricular septal defects) can be assessed by oximetry runs in a systematic fashion. However, this assumes incorrectly complete shunting at each level, and thus represents a potential source of error.
Specific conditions
The aim of this section is to inform the cardiologist dealing with adults what to look for, when diagnostic catheterisation is performed in patients with congenital heart conditions. Relevant interventional procedures are discussed in specific chapters. It is worth noting that the following paragraphs on catheterisation in grown-up congenital heart disease can by no means be considered complete, but they focus on some topics relevant to grown-up congenital heart disease.
REPAIRED COARCTATION ( View chapter )
Whereas surgical repair of aortic coarctation can be performed with a low mortality and morbidity, re-coarctation or residual stenosis is seen not infrequently in adult patients post surgical repair. Catheterisation in these patients should include a thorough haemodynamic assessment with simultaneous pressure measurements proximal and distal to the site of surgical repair with the recording of pullback gradients. We recommend angiography with the catheter (pigtail) positioned at the level of the aortic arch (in frontal and lateral projection or modified depending on the anatomy). Aortic angiography gives information about diameters at the level of obstruction and possible post-surgical aortic (pseudo-) aneurysms. Also, angiography provides information on the morphology of the aortic arch, which can be hypoplastic and thus possibly representing the more relevant level of obstruction. Head and neck vessels can be visualised, with variations in anatomy and function, also depending on the surgical technique for initial repair (subclavian flap repair vs. end-to-end-repair vs. interposition of conduits). As coarctation of the aorta may be associated with dilatation of the ascending aorta, this should be excluded/confirmed on angiography.
Balloon angioplasty and stenting of aortic coarctation will be discussed in a different chapter.
Considerations for diagnostic catheterisation in repaired coarctation
- Gradient across the site of repair
- Dimensions and anatomy (aneurysm, residual stenosis) at the level of repair
- Presence of collaterals
- Assessment of the aortic arch (especially the presence of hypoplasia or additional stenosis)
- Anatomy of head and neck vessels (including their origin in relation to residual lesions)
- Dilatation of the ascending aorta
- Presence of a bicuspid aortic valve, valvar stenosis or regurgitation
- Ventricular function
BRANCH PULMONARY ARTERY STENOSIS
Residual or postoperative branch pulmonary artery stenosis is frequent in children and adults with congenital heart disease. Branch pulmonary artery stenosis can be related to the congenital condition, as an isolated lesion or in association with valvar pulmonic stenosis, septal defects, tetralogy of Fallot, or syndromes such as Williams, Noonan or Alagille. Branch pulmonary artery stenosis is also seen post- surgical shunt placement. Shunt placement to either left or right pulmonary artery can lead to distortion and upwards traction of the pulmonary branches during somatic growth, resulting in a significant obstruction.
Haemodynamics should be assessed as outlined previously. For a first impression of branch pulmonary artery anatomy, pulmonary angiography in frontal and lateral projection should be acquired. The bifurcation is best visualised using frontal cranial projections. The right pulmonary artery is best seen in the AP view and the left pulmonary artery in the left anterior oblique view with cranial angulation.
Whereas surgical patching of stenotic arteries is usually performed during neonatal or repeated surgery, residual obstruction in children and adults and severe distal stenosis are best treated by balloon angioplasty with or without stenting.
Using high-pressure balloons about 2 to 3 times bigger than the size of the smallest vessel, a success rate (defined by a 50% or larger increase in diameter) of ~75% has been reported [1111. Gentles TL, Lock JE, Perry SB. High pressure balloon angioplasty for branch pulmonary artery stenosis: early experience. J Am Coll Cardiol. 1993;22:867-72. ].
However, there is an incidence of recurrent narrowing after balloon angioplasty of about 17%, which could be related to the elastic recoil of the pulmonary artery wall. The efficacy of endovascular stents to relieve such obstructions and the safety of their implantation has been demonstrated with a success rate above 96% [1212. Mullins CE, O’Laughlin MP, Vick GW 3rd, Mayer DC, Myers TJ, Kearney DL, Schatz RA, Palmaz JC. Implantation of balloon-expandable intravascular grafts by catheterization in pulmonary arteries and systemic veins. Circulation. 1988;77:188-99.
An early report on the use of stents in congenital heart disease., 1313. O’Laughlin MP, Perry SB, Lock JE, Mullins CE. Use of endovascular stents in congenital heart disease. Circulation. 1991;83:1923-39.
An early report on the use of stents in congenital heart disease., 1414. Benson LN, Hamilton F, Dasmahaptra H, Rabinowitch M, Coles JC, Freedom RM. Percutaneous implantation of a balloon-expandable endoprosthesis for pulmonary artery stenosis: An experimental study. J Am Coll Cardiol. 1991;18:1303-8. ]. If obstructions are near to the bifurcation or side branches, simultaneous implantation of stents is recommended ( Figure 4 ) [1515. Stapleton GE, Hamzeh R, Mullins CE, Zellers TM, Justino H, Nugent A, Nihill MR, Grifka RG, Ing FF. Simultaneous stent implantation to treat bifurcation stenoses in the pulmonary arteries: Initial results and long-term follow up. Catheter Cardiovasc Interv. 2009;73:557-63. ]. In specific lesions a cutting balloon may be useful.
Major complications are seldom encountered, but include death from pulmonary artery embolism, vascular rupture, pulmonary bleeding and embolisation of incorrectly placed stents [1616. Moore JW, Spicer RL, Perry JC, Mathewson JW, Kirkpatrick SE, George L, Uzark K, Mainwaring RL, Lamberti JJ. Percutaneous use of stents to correct pulmonary artery stenosis in young children after cavopulmonary anastomosis. Am Heart J. 1995;130:1245-9. , 1717. Hijazi ZM, Al-Fadzey F, Geggel RL, Marx GR, Galal O, al-Halees Z, Abbag F, Fulton DR. Stent implantation for relief of pulmonary artery stenosis: Immediate and short-term results. Cathet Cardiovasc Diagn. 1996;36:16-23. ]. Compression of coronary arteries may also occur and must be excluded by simultaneous test-balloon dilation and coronary angiography [1818. Gewillig M, Brown S. Coronary compression caused by stenting a right pulmonary artery conduit. Catheter Cardiovasc Interv. 2009;74:144-7. ]. Bronchial compression has been described [1919. Moszura T, Mazurek-Kula A, Dryzek P, Sysa A. Bronchial compression as adverse effect of left pulmonary artery stenting in a patient with hypoplastic left heart syndrome. Pediatr Cardiol. 2010;31:530-3. ].
TETRALOGY OF FALLOT
After neonatal surgical repair of tetralogy of Fallot, residual lesions impacting on ventricular size, function, symptoms, exercise performance and risk of arrhythmia and sudden death are frequent [2020. Apitz C, Webb GD, Redington AN. Tetralogy of Fallot. Lancet. 2009;374:1462-71.
A very nice review on tetralogy of Fallot summarising the variety of clinical, morphological and pathophysiological features in adulthood.]. Residual lesions comprise right ventricular dilatation and dysfunction, residual shunting across the surgically patched ventricular septal defect, branch pulmonary artery stenosis, right ventricular outflow tract aneurysm ( Figure 5 ) and severe pulmonary regurgitation (especially after transannular patching) [2121. Kalra N, Klewer SE, Raasch H, Sorrell VL. Update on tetralogy of Fallot for the adult cardiologist including a brief historical and surgical perspective. Congenit Heart Dis. 2010;5:208-19. ]. Left ventricular dysfunction and dilatation of the aortic root can also be seen in adults long after surgical correction.
In these patients, catheterisation represented the diagnostic gold standard for decades. However, with advances in non-invasive imaging techniques such as echocardiography and magnetic resonance imaging in particular, the number of diagnostic catheterisations in adults with tetralogy of Fallot is decreasing at most centres.
The catheterisation protocol should include assessment of residual shunting by oximetry runs, right ventricular angiography for determination of systolic function and degree of dilatation, and pulmonary angiography to visualise and judge pulmonary regurgitation and residual branch pulmonary artery stenosis, if present. Furthermore, on left ventricular angiography, residual shunting across the ventricular septal defect patch and possible dilatation of the aortic root can be visualised.
Considerations for diagnostic catheterisation in repaired tetralogy of Fallot
- Right ventricular size and function
- Degree of tricuspid regurgitation
- Dimensions of and gradient across the right ventricular outflow tract (obstruction/dilatation)
- Qualitative and and semiquantified assessment of pulmonary regurgitation
- Anatomy of branch pulmonary arteries
- Presence of a residual ventricular septal defect
- Presence of dilatation of the aortic root
TRANSPOSITION OF THE GREAT ARTERIES
Post arterial switch procedure
During the arterial switch procedure, the aorta and pulmonary artery are disconnected and their positions are then ‘‘switched’’. The aorta is stitched to the former pulmonary trunk arising from the left ventricle and the pulmonary artery connected to the aortic root originating from the right ventricle. Furthermore, the pulmonary bifurcation is brought in front of the neo-ascending aorta (‘’Lecompte manoeuvre’’) [2222. Lecompte Y, Zannini L, Hazan E, Jarreau MM, Bex JP, Tu TV, Neveux JY. Anatomic correction of transposition of the great arteries. J Thorac Cardiovasc Surg. 1981;82:629-31. ], obviating the need for interposition conduits in pulmonary position. Atrial and ventricular septal defects are closed, if present. The major challenge of the procedure is the liberation of the coronary arteries from their origins and tension-free reinsertion to the neo-aorta using a “button” technique [2323. Mee RBB. The Arterial Switch Operation. In: Stark J, De Leval M, Tsang VT, eds. Surgery for congenital heart defects. 3rd ed. Chichester; Hoboken, NJ: John Wiley & Sons; 2006. xxxiv, 718 p. ].
Whereas long-term outcome data about this procedure is generally favourable it is still limited. Complications in children and adults with transposition of great arteries and the arterial switch procedure are mainly related to the surgical steps described above [2424. Tobler D, Williams WG, Jegatheeswaran A, Van Arsdell GS, McCrindle BW, Greutmann M, Oechslin EN, Silversides CK. Cardiac outcomes in young adult survivors of the arterial switch operation for transposition of the great arteries. J Am Coll Cardiol. 2010;56:58-64. , 2525. Murphy DJ Jr. Transposition of the great arteries: long-term outcome and current management. Curr Cardiol Rep. 2005;7:299-304.
One of the most important papers on late outcome and current management after transposition of the great arteries.].
During catheterisation, selective coronary angiograms should be performed, since surgical re-insertion of coronaries into the neo-aorta might subsequently lead to ostial or proximal coronary artery stenosis [2626. Bonhoeffer P, Bonnet D, Piechaud JF, Stumper O, Aggoun Y, Villain E, Kachaner J, Sidi D. Coronary artery obstruction after the arterial switch operation for transposition of the great arteries in newborns. J Am Coll Cardiol. 1997;29:202-6. ]. The patch repair where the coronary ostia were harvested from the neo-pulmonary trunk, and the translocation of the pulmonary artery can cause obstruction of the main pulmonary artery or the bifurcation, which is excluded or confirmed on haemodynamic measurements. The ‘’Lecompte manoeuvre’’ may lead to kinking of the branch pulmonary artery on its course around the ascending aorta. Therefore, possible gradients should be detected, and the degree of obstruction determined by angiography. The circular supravalvular anastomoses of pulmonary artery and aorta are rarely stenotic. Sometimes the neo-aortic root tends to dilate over time.
Finally, possible distortion of the neo-pulmonary and aortic valve can result in regurgitation and is examined on angiography accordingly.
Considerations for diagnostic catheterisation post arterial switch procedure
- Function of the neo-aortic and neo-pulmonary valves
- Transposed coronary arteries : assessment of possible coronary stenosis (ostial, proximal)
- Aortic root: assessment for possible dilatation
- Pulmonary and aortic anastomosis: assessment for possible supravalvular stenosis
- Pulmonary bifurcation and branch pulmonary arteries: anatomy and possible gradients
Post atrial switch procedure
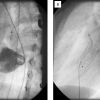
Atrial switch procedures (Mustard and Senning) were routinely performed as a physiological correction for transposition of the great arteries before the techniques of anatomical arterial switch repair were established. By means of an ingenious atrial “baffle”, the flow from the caval veins was directed towards the mitral valve and the flow from the pulmonary veins to the tricuspid valve. The transposition of the great arteries itself remained unchanged. Thus in these patients the right ventricle remains the systemic ventricle while the left ventricle supports pulmonary circulation. In order to correctly identify the anatomy, atria should not be called “right” and “left” but “systemic venous” and “pulmonary venous” in this condition. On cardiac catheterisation, typical late problems following this type of repair which need to be screened for are: (i) inflow-obstructions from the caval or pulmonary veins to the respective atria ( Figure 6 & Figure 7 ); (ii) very atypical interatrial “baffle” defects; (iii) tricuspid regurgitation; and (iv) right ventricular dysfunction. Both leaks and obstruction of baffles can be treated with intervention by implantation of stents or plugs [2828. Witsenburg M, Qureshi S, Carminati M, Gewillig, Brezinska-Raiszys, Szatmari A. Recommendations from the Association for Paediatric Cardiology for training in diagnostic and interventional cardiac catheterization. Cardiol Young. 2010;20:470-2. ]. Today, the atrial switch is reserved for more complex lesions and performed as part of the “double switch” repair for congenitally corrected transposition of the great arteries (double discordance).
Considerations for diagnostic catheterisation post atrial switch procedure
- Assessment of right (systemic) ventricular function
- Assessment of tricuspid regurgitation
- Assessment for obstruction of the systemic and/or pulmonary venous return
- Presence of a left to right shunt or right to left shunt (including their location and size)
- Presence of a compromised coronary sinus
- Presence of left ventricular outflow tract obstruction
AORTOPULMONARY SHUNTS
In the past (and in the absence of corrective alternatives) aortopulmonary shunts were developed for the palliation of cyanotic lesions with diminished pulmonary blood flow. The classic “Blalock-Taussig” shunt was a direct anastomosis of the proximal part of a distally sacrificed subclavian artery to the ipsilateral pulmonary artery. The “Waterston” shunt was a direct window-like anastomosis between the ascending aorta and the right pulmonary artery while the “Potts” shunt was its equivalent between the descending aorta and the left pulmonary artery. Typical complications included either a large shunt with unrestricted pulmonary blood flow leading to pulmonary oedema, heart failure and subsequently increased pulmonary vascular resistance, or stenosis/occlusion of pulmonary branch arteries. Sometimes both problems developed in either lung. Today, aortopulmonary shunts have all but been abandoned for corrective procedures and are performed only for temporary palliation of duct dependent lesions: a polytetrafluoroethylene (PTFE)-tube with a diameter from 3 to 4 mm is inserted end-to-side between the brachiocephalic trunk and respective subclavian artery and ipsilateral pulmonary artery (modified Blalock-Taussig shunt) or between the ascending artery and pulmonary trunk (central shunt). The interventional equivalent is stent implantation to the arterial duct. In special situations some centres prefer ventriculopulmonary shunts (Sano shunt).
In patients who underwent shunt palliation in infancy, residual shunting and branch pulmonary artery stenosis have to be excluded since elevated pulmonary vascular resistance may be present. Shunt obstruction may occur due to localised stenosis or intimal proliferation, and balloon dilatation or stenting may help to solve such problems.
VENOUS SHUNTS AND THE CONCEPT OF UNIVENTRICULAR PALLIATION
The classic upper cavopulmonary anastomosis was developed as an alternative to the complications of aortopulmonary shunts and consisted of direct end-to-end anastomosis of the superior caval vein to the ipsilateral (usually right) pulmonary artery (unilateral unidirectional Glenn anastomosis). This long-abandoned procedure frequently led to the development of venovenous fistulas resulting in an intrapulmonary right to left shunt. Vascular plugs are useful for occluding these vessels.
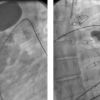
Contemporary treatment of anatomically or functionally univentricular hearts consists of step-by-step separation of the pulmonary and systemic circulation leaving pulmonary blood flow without an upstream pumping chamber. The first step is performed in the newborn: depending on anatomy, pulmonary blood-flow is maintained/established by either aortopulmonary shunts or restricted by pulmonary artery banding (shunt or occlusion respectively). The second step performed at an age of four to six months consists of an upper cavopulmonary shunt with an end-to-side anastomosis between the distal part(s) of the transected superior caval vein(s) and the ipsilateral pulmonary artery (unilateral or bilateral bidirectional Glenn anastomosis respectively). A modification called “Hemi-Fontan” consists of an additional anastomosis of the proximal part of the superior caval vein to the pulmonary artery and patch occlusion at the entry to the atrium. The third step performed at an age of about three years is named “Fontan” and consists of additionally directing the inferior caval flow to the pulmonary artery. The concept underwent many modifications over time and today it is either performed as extra-atrial conduit or intra-atrial tunnel ( Figure 8 ). Typical vascular complications of these venous shunts are the development of veno-venous collaterals and occasional intrapulmonary arteriovenous fistulas ( Figure 9 ). Stenoses may occur at various locations and may have to be treated aggressively. If the right atrium is part of the Fontan pathway, it tends to dilate severely and may be the origin of subsequent arrhythmias.
Conclusion
Cardiac catheterisation remains an essential technique in diagnosis and treatment of children and adults with grown-up congenital heart disease. Although there are some standardised catheterisation procedures similar to those in acquired heart disease, there is no general catheter approach to congenital cardiovascular malformations. Each catheterisation has to be considered as an individual case in order to meet the often unique anatomical and physiological situations of these patients. Sound knowledge of a patient’s history, clinical data and non-invasively acquired information is crucial for the success of cardiac catheterisations in patients with complex congenital heart disease or its sequelae following corrective or palliative treatment [2828. Witsenburg M, Qureshi S, Carminati M, Gewillig, Brezinska-Raiszys, Szatmari A. Recommendations from the Association for Paediatric Cardiology for training in diagnostic and interventional cardiac catheterization. Cardiol Young. 2010;20:470-2. ].
Personal perspective – Philipp Bonhoeffer
With improvement in prenatal diagnosis, perinatal management, cardiac surgery, non-invasive imaging and intensive care, the number of patients with congenital heart disease surviving to adulthood has increased significantly over recent decades [2929. Marelli AJ, Mackie AS, Ionescu-Ittu R, Rahme E, Pilote L. Congenital heart disease in the general population: changing prevalence and age distribution. Circulation. 2007;115:163-72. ]. As a result, the heterogeneity and complexity of these patients, who underwent multiple surgical and interventional procedures, will equally increase. This represents an enormous clinical challenge. Catheterisation, whether for diagnostic or interventional purposes, requires a fair amount of experience, flexibility and creativity to deal with unique and sometimes unexpected problems. Whereas some diagnostic catheterisations in this patient population have been replaced by three-dimensional imaging modalities, the number of catheter-based interventions is likely to increase with introduction of new techniques such as percutaneous pulmonary valve implantation [3030. Lurz P, Coats L, Khambadkone S, Nordmeyer J, Boudjemline Y, Schievano S, Muthurangu V, Lee TY, Parenzan G, Derrick G, Cullen S, Walker F, Tsang V, Deanfield J, Taylor AM, Bonhoeffer P. Percutaneous pulmonary valve implantation: impact of evolving technology and learning curve on clinical outcome. Circulation. 2008;117:1964-72. ].








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}