



Case presentation
The case was a native LAD CTO, characterized by tapering proximal cap, uplifted proximal LAD segment due to graft anastomosis, short occlusion length, poor distal landing zone, calcification, and retrograde filling through a LIMA to LADDg to LAD ( Video 1). Prior PCI attempt was made bilaterally via a LIMA graft to LADDg to LAD as retrograde access, but reverse CART did not succeed with knuckle wiring for overlapping in the CTO, nor did direct crossing. So, deflection wiring was planned for a second attempt, with an antegrade Gaia 2 navigated to a LADDg direction using "clockwise" rotation ( Video 2), while a retrograde Gaia 2 over a Caravel 150 cm via LIMA graft deflected "counter-clockwise" to get proximity with the other wire ( Video 3).
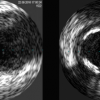
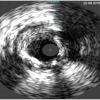
The tips of the wires seemed overlapping in the RAO cranial and caudal projections, where a 1.5 mm balloon dilated to implement reverse CART ( Figure 1). IVUS revealed a retrograde wire in an edge of the subintimal ( Figure 2 a), but a little distal site disclosed a wire intraluminal ( Figure 2 b). Therefore, a retrograde Caravel advanced in the nearest place, where the wire was exchanged to a Fielder XT-R with a minimal bend (< 1.0mm) and shallow angle of 30°, which successfully enter an antegrade guide ( Video 4) along with a microcatheter.
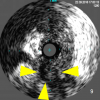
The wire was exchanged for an RG3 for externalization. After 1.5 mm balloon dilation throughout the occlusion, IVUS confirmed an intimal tracking (in the proximal CTO ( Figure 3) and the ostial LADDg ( Figure 4), and a second workforce wire was placed into the distal LAD via a Fine duo (a double lumen microcatheter, Terumo, Japan, Video 5), over which additional balloon dilatation and DES deployment over the diseased segments resulted in an excellent result ( Video 6).
The case highlighted a narrow window of calcified and distorted post-operative native LAD CTO, where deflection control of an antegrade and a retrograde wire facilitated a directed reverse CART possible, keeping an intimal wire tracking through a complex occlusion.


{kind=link}
{kind=link}
{kind=link}
{kind=link}