Summary
Atrial transseptal puncture was developed to provide precise left heart haemodynamics for the assessment of valve disease. This use was replaced by echocardiography, but it continued to be used for aortic and mitral balloon valvotomy and left heart pathway ablations. During the last 10 years, the role of transseptal puncture has increased greatly for atrial fibrillation ablations, transcatheter repair of mitral regurgitation, closure of some patent foramen ovales, left atrial appendage obliteration, paraprosthetic valve leak repair, positioning of left ventricular assist devices, pulmonary vein stenting and resynchronisation therapy. This resurgence has been accompanied by new devices and variations in the classic technique. While fluoroscopy is still largely used to guide transseptal puncture, intraprocedure echocardiography has become widely used in specific interventions.
Introduction
The objective of atrial transseptal puncture is the safe and effective delivery of catheterisation equipment from the right atrium (RA) to the left heart. It was introduced into clinical practice in 1959 by Ross, Morrow and Braunwald [11. Ross J, Jr. Transeptal left heart catheterization: a new method of left atrial puncture. Ann Surg. 1959;149:395-401. , 22. Ross J, Jr., Braunwald E, Morrow AG. Transseptal left atrial puncture; new technique for the measurement of left atrial pressure in man. Am J Cardiol. 1959;3:653-5. ]. Its initial use was to provide precise haemodynamic measurements to help in the selection of patients for cardiac valve surgery. It allowed simultaneous measurement of pressure gradients across the mitral and aortic valves. Forward and backward indocyanine green dye curves permitted calculation of cardiac output and valvular regurgitant fraction. Technically speaking, Manfredi [33. Manfredi D. [New catheter in the study of physiology of the left heart]. Arch Ital Chir. 1956;81:409-16. ] described the use of a curved transseptal catheter/needle in 1956 and Cope, the use of a straight needle in 1959 [44. Cope C. Technique for transseptal catheterization of the left atrium; preliminary report. J Thorac Surg. 1959;37:482-6. ]. Before the introduction of transseptal puncture, left atrial (LA) pressure was available only available by more uncomfortable techniques, such as needle puncture from the suprasternal notch (Radner technique) [55. Radner S. Suprasternal puncture of the left atrium for flow studies. Acta Med Scand. 1954;148:57-60. ], via bronchoscopy [66. Allison PR, Linden RJ. The bronchoscopic measurement of left auricular pressure. Circulation. 1953;7:669-73. , 77. Facquet J, Lemoine JM, Alhomme P, Lefebvre J. Transbronchial measurement of left auricular pressure. Arch Mal Coeur Vaiss. 1952;45:741-5. ] or by a paravertebral approach [88. Bagger M, Bjork VO, Malmstrom G. Technique and sequelae of catheterization of the left side of the heart. Am Heart J. 1957;53:91-9. ]. Intercostal puncture into the left ventricle [99. Brock R, Milstein BB, Ross DN. Percutaneous left ventricular puncture in the assessment of aortic stenosis. Thorax. 1956;11:163-71. ] could also be used for gradient recording in patients with aortic stenosis. These earlier techniques had a surprisingly good safety record [1010. Carr PW, Roach EA, Mudd JG. Percutaneous suprasternal puncture (Radner technique) of the left ventricle: a report of 646 cases. Dis Chest. 1967;52:676-9. ], reflecting the body’s tolerance of a thin sterile needle because of the elastic recoil of the tissues.
With the progressive development of echocardiographic imaging and Doppler measurements, the use of atrial transseptal puncture declined. However, it was continued in the 1980s for mitral balloon valvotomy [1111. Vahanian A, Michel PL, Cormier B, Vitoux B, Michel X, Slama M, Sarano LE, Trabelsi S, Ben Ismail M, Acar J. Results of percutaneous mitral commissurotomy in 200 patients. Am J Cardiol. 1989;63:847-52. ] and antegrade aortic stenosis balloon dilatation [1212. Bahl VK, Chandra S, Goswami KC, Manchanda SC. Balloon aortic valvuloplasty in young adults by antegrade, transseptal approach using Inoue balloon. Cathet Cardiovasc Diagn. 1998;44:297-301. ]. Since the turn of the century, there has been a major resurge in its use. At present, by far the most common indication is left heart electrophysiological (EP) ablations, but it is also being used for a variety of new interventional procedures, including percutaneous mitral valve repair, some patent foramen ovale (PFO) closures, left atrial appendage (LAA) occlusion, paraprosthetic valve leak repair, percutaneous valve-in-valve and valve-in-ring implantation [1313. Bouleti C, Fassa AA, Himbert D, Brochet E, Ducrocq G, Nejjari M, Ghodbane W, Depoix JP, Nataf P, Vahanian A. Transfemoral implantation of transcatheter heart valves after deterioration of mitral bioprosthesis or previous ring annuloplasty. JACC Cardiovasc Interv. 2015;8:83-91. ] and for positioning of left ventricular assist devices within the LA. It is also still very occasionally used for diagnosis ( Table 1 ). Until recently, the emphasis had been on achieving a safe transseptal puncture at the fossa ovalis, but the new interventional techniques often require a more precise location of the crossing point within the atrial septum. This has led to an increasing use of echocardiographic imaging guidance in addition to fluoroscopy for these procedures, which has also increased safety..
Equipment
Transseptal puncture is possible because the right femoral vein is large and straight enough to allow passage of a needle that has a distal curve sufficient to turn towards the atrial septum. The proximal hub of the stainless steel needle has an arrow which corresponds to the direction of the curve ( Figure 1 ).
The original Ross needle was modified by Brockenbrough [1414. Brockenbrough EC, Braunwald E, Ross J, Jr. Transseptal left heart catheterization; A review of 450 studies and description of an improved technic. Circulation. 1962;25:15-21. , 1515. Brockenbrough EG, Braunwald E. A new technic for left ventricular angiocardiography and transseptal left heart catheterization. Am J Cardiol. 1960;6:1062-4. ] by reducing the calibre of the needle from 18 to 21 gauge in its distal 1.5 cm. This gave greater safety in the event of any needle puncture outside the LA cavity. The catheter was also modified to include side-holes near the distal tip to allow better and safer injection of contrast. The Brockenbrough catheter and needle have retained these same design features to the present day. However, increasing use has been made of the Mullins transseptal catheter. It has a tight-fitting outer sheath, which can be used to deliver other catheters (e.g., Swan-Ganz balloon catheters) to the left heart. The Mullins catheter has a more tapered tip than the Brockenbrough catheter and there is a reduced protrusion of the Brockenbrough needle ( Figure 2 ).
The needle is not a surgical instrument and its long lumen means that adequate cleaning cannot be assured, so re-sterilisation is not recommended. Several manufacturers now produce these transseptal sets, usually with only minor variations in design [1616. Leon-Sit P, Callans D. Equipment for transseptal punctures. In: Thakur R, Natale A, eds Transseptal Catheterisation and Interventions. Minneapolis: Cardiotext Publishing; 2010:55-64. ]. The “historical” Brockenbrough needle (Medtronic, Minneapolis, Minnesota) presented in Figure 1 is available in one size. However, other manufacturers have developed transseptal needles with different angulations, such as the BRK series (St. Jude Medical, St Paul, Minnesota, USA) ( Figure 3 ). “ES” extra-sharp versions have also been developed to facilitate septum crossing. Paediatric versions are also marketed. With both Brockenbrough and Mullins catheters, there are versions with wider curves of the catheter/sheath to assist crossing the mitral valve in the presence of an enlarged LA ( Figure 4 ). Other sheaths of various shapes and sizes have been developed more recently to allow LAA access according to specific indications [1717. Alkhouli M, Rihal CS, Holmes DR, Jr. Transseptal Techniques for Emerging Structural Heart Interventions. JACC Cardiovasc Interv. 2016;9:2465-80. ].
The Endrys transseptal coaxial double-needle system (Cook Europe, Bjaeverskov, Denmark) is used by some, particularly when there is a small LA and the very thin inner needle is felt to improve safety ( Figure 5 ).
Contraindications to transseptal puncture
The following are usually listed as contraindications to transseptal puncture:
- LA thrombus or tumour
- distorted anatomy due to congenital heart disease
- significant chest or spine deformity
- the inability to lie flat
- ongoing anticoagulation
- marked atrial enlargement
- dilated aortic root
- previous patch repair of the atrial septum.
However, of these, the only absolute contraindications to transseptal puncture are a thrombus located at the septum and an atrial myxoma or other tumour arising from the septum. The other conditions make transseptal puncture more difficult, but are regularly dealt with by experienced operators. The presence of structural abnormalities makes additional information from intra-procedural echocardiography very helpful.
Transoesophageal echocardiography (TOE) is indicated prior to transseptal puncture when there is structural heart disease or chronic atrial fibrillation (AF) in order to look for atrial thrombus. The presence of any LA thrombus always calls for great caution because of the danger of causing embolism. Normally any left heart procedure is contraindicated when any atrial thrombus is present. Occasionally, mitral balloon valvotomy has been successfully performed when the thrombus is located well within the LAA and is non-mobile [1818. Shaw TR, Northridge DB, Sutaria N. Mitral balloon valvotomy and left atrial thrombus. Heart. 2005;91:1088-9. ]. However, it can only be indicated in patients who are candidates for urgent life-saving intervention but not surgery. Most atrial thrombi will resolve over 3-6 months of intensive anticoagulation (aiming for an INR 3.5-4.5). The performance of the procedure can therefore be differed and performed safely if repeat TOE confirms the thrombus has resolved.
Transseptal puncture through an intra-atrial patch has been found to be a safe procedure [1919. El-Said HG, Ing FF, Grifka RG, Nihill MR, Morris C, Getty-Houswright D, Mullins CE. 18-year experience with transseptal procedures through baffles, conduits, and other intra-atrial patches. Catheter Cardiovasc Interv. 2000;50:434-9; discussion 40. ]. Successful puncture in the presence of an Amplatz septal occluder has also been reported [2020. Cook S, Meier B, Windecker S. Transseptal TandemHeart implantation through an Amplatzer atrial septal occluder. J Invasive Cardiol. 2007;19:198-9. , 2121. Pedersen ME, Gill JS, Qureshi SA, Rinaldi CA. Successful transseptal puncture for radiofrequency ablation of left atrial tachycardia after closure of secundum atrial septal defect with Amplatzer septal occluder. Cardiol Young. 2010;20:226-8. ].
When the heart is displaced by pulmonary changes, the inferior vena cava (IVC) does not follow a normal path, and the alignment of the catheter/needle and the LA cavity may be much altered: additional information from contrast injection/echocardiography is then particularly helpful.
With azygous continuation of the IVC, venous drainage from the lower body does not join the inferior surface of the RA, but continues to enter near the superior vena cava (SVC). This uncommon anomaly makes transseptal puncture from the IVC impossible and an SVC or transhepatic approach is required. It should be diagnosed by X-ray before the procedure or if, during the procedure, the catheter has an unusually posterior position behind the heart ( Figure 6 ), confirmed by venous angiography in the RA [2222. Attias D, Himbert D, Redheuil A, Brochet E, Mousseaux E, Blanc J, Lung B, Vahanian A. A pitfall of transseptal catheterisation for percutaneous mitral commissurotomy: interruption of the inferior vena cava with azygos continuation. Arch Mal Coeur Vaiss. 2007;100:64-7. ].
Complex congenital diseases are also considered contra-indicative for transseptal puncture due to the altered anatomical landmarks.
Transseptal catheterization can be performed in dextrocardia by experienced operators using left femoral access, inversion of the X-ray image and echocardiographic guidance [2323. Nallet O, Lung B, Cormier B, Porte JM, Garbarz E, Michel PL, Vahanian A. Specifics of technique in percutaneous mitral commissurotomy in a case of dextrocardia and situs inversus with mitral stenosis. Cathet Cardiovasc Diagn. 1996;39:85-8. ].
Obstruction of the vena cava is a classic contraindication for femoral access, but membranous obstruction of the vena cava can be dilated. An IVC filter does not necessarily preclude transseptal puncture via the femoral vein if flow is still present in the IVC, as the equipment is slim enough to pass through most models.
If there is marked osteoarthritic change in the lumbar spine, the needle curve may refuse to be advanced across the iliac crest. This can be overcome by partially withdrawing the catheter, re-advancing the needle to the point of resistance and the forward movement of the catheter then carries the needle past the obstruction.
Thoracic deformity, such as kyphoscoliosis, is a contraindication if severe. In practice, the level of acceptable deformity depends on operator experience. Echocardiographic guidance can overcome this difficulty.
Transseptal catheterisation should be avoided, if possible, in a patient with a bleeding diathesis or an INR >1.5 (in particular in patients who have not undergone previous cardiac operation).
When intravenous heparin is used, it should be discontinued 4 hours before and can be restarted 2 hours after the procedure. This rule has been challenged in two circumstances where the risk of thrombosis resulting from the withdrawal of anticoagulation in lengthy procedures may be worse than that of bleeding. Firstly, in MitraClip implantation, when it is performed by experienced operators under TOE, it is possible to perform transseptal puncture with an INR >2 [2424. Boekstegers P, Hausleiter J, Baldus S, von Bardeleben RS, Beucher H, Butter C, Franzen O, Hoffmann R, Ince H, Kuck KH, Rudolph V, Schafer U, Schillinger W, Wunderlich N, Germany Society of Cardiology Working Group on Interventional Cardiology Focus Group on Interventional Mitral Valve Therapy. Percutaneous interventional mitral regurgitation treatment using the Mitra-Clip system. Clin Res Cardiol. 2014;103:85-96. ]. Secondly, the same opinion is shared by electrophysiologists planning transseptal puncture before AF ablation because of the long duration of the procedure, the presence of AF and the thrombotic effect of radiofrequency (RF) lesion, clotting in the LA and/or on the transseptal sheath and ensuing stroke are always feared. Hence, most EP centres now perform transseptal puncture and catheter ablation of AF without warfarin discontinuation and with heparin on top of vitamin K antagonists, which reduces the occurrence of periprocedural stroke and minor bleeding complications. During AF ablation procedures, heparin is administered prior to, or immediately following, transseptal puncture and adjusted to achieve and maintain an activated clotting time of 300-400 seconds throughout the procedure [2525. Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA, Crijns HJ, Damiano RJ, Jr., Davies DW, DiMarco J, Edgerton J, Ellenbogen K, Ezekowitz MD, Haines DE, Haissaguerre M, Hindricks G, Iesaka Y, Jackman W, Jalife J, Jais P, Kalman J, Keane D, Kim YH, Kirchhof P, Klein G, Kottkamp H, Kumagai K, Lindsay BD, Mansour M, Marchlinski FE, McCarthy PM, Mont JL, Morady F, Nademanee K, Nakagawa H, Natale A, Nattel S, Packer DL, Pappone C, Prystowsky E, Raviele A, Reddy V, Ruskin JN, Shemin RJ, Tsao HM, Wilber D. 2012 HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Europace. 2012;14:528-606. , 2626. Di Biase L, Burkhardt JD, Santangeli P, Mohanty P, Sanchez JE, Horton R, Gallinghouse GJ, Themistoclakis S, Rossillo A, Lakkireddy D, Reddy M, Hao S, Hongo R, Beheiry S, Zagrodzky J, Rong B, Mohanty S, Elayi CS, Forleo G, Pelargonio G, Narducci ML, Dello Russo A, Casella M, Fassini G, Tondo C, Schweikert RA, Natale A. Periprocedural stroke and bleeding complications in patients undergoing catheter ablation of atrial fibrillation with different anticoagulation management: results from the Role of Coumadin in Preventing Thromboembolism in Atrial Fibrillation (AF) Patients Undergoing Catheter Ablation (COMPARE) randomized trial. Circulation. 2014;129:2638-44. ].
Except in the specific cases described above, a bolus heparin dose of 3,000–5,000 units or up to 100 units per kg body weight is usually used.
Conditions when transseptal puncture should not be undertaken
- Thrombus at septum
- Atrial myxoma
- Tumour at septum
- Left atrial thrombus (usually)
- Bleeding diathesis
Imaging before the procedure
A transthoracic echocardiogram (TTE) gives a good and important overview of the cardiac structures and their function. The apical four-chamber view shows the thickness and curvature of the atrial septum and the size of the atrial cavities as well as abnormalities, such as atrial septum aneurysm or atrial myxoma. In addition, the presence of even a mild-to-moderate pericardial effusion should be described in the echo report in order to serve as a comparator if haemopericardium is suspected during the procedure.
While transthoracic views can reveal atrial thrombus, they cannot be used to exclude its presence, particularly in the atrial appendage. The performance of TOE is therefore recommended for all patients due to undergo transseptal puncture, although it is often not performed before EP procedures with a normal size of LA in a patient considered at low risk of thrombus. When a patient is being referred to another centre for mitral valvuloplasty, it is worth considering a prereferral TOE to check for atrial thrombus requiring a period of intensive anticoagulation. Even if no thrombus is shown, the TOE would be repeated just prior to the valvuloplasty unless the pre-referral TOE has been very recent e.g., within 2 weeks.
Transseptal puncture technique
The patient lies supine on the table unless in pulmonary oedema. A peripheral intravenous catheter is in place for drug/fluid administration.
There is no single way to perform atrial transseptal puncture. In practice, almost all operators follow the practice of their training mentor and build up their own experience of that particular approach.
Fluoroscopic guidance
The puncture can be undertaken using any of four fluoroscopic positions, preferably in combining two of them.
ANTEROPOSTERIOR
This was the fluoroscopic projection used in the initial descriptions of the procedure. Many operators still prefer this projection as it is the fluoroscopic view with which they are most familiar, and it gives a good overall view of the cardiac silhouette and lung fields.
When transseptal puncture was first used, the catheter was advanced over a guidewire to the RA cavity. With the wire withdrawn, the needle was then advanced through the catheter, taking care to allow the needle to turn and twist without hindrance as it advanced to the catheter tip. The catheter/needle was then rotated towards the LA, as judged by fluoroscopy, and the needle advanced.
In 1965, Bloomfield and Sinclair-Smith [2727. Bloomfield DA, Sinclair-Smith BC. The Limbic Ledge. A Landmark for Transseptal Left Heart Catheterization. Circulation. 1965;31:103-7. ] described a way in which the limbic edge, the ridge where the septum secundum overlies and usually fuses with the septum primum, could be identified. They passed the catheter over a wire to the SVC. The needle was advanced to lie just within the catheter tip. In the past, the distance between the needle hub and the catheter hub when the needle was just within the catheter was noted and marked. With modern fluoroscopy equipment, this is not needed. The needle curve is directed to 4 o’clock (as seen from below), or up to 6 o’clock for a very dilated LA. The catheter/needle is then slowly withdrawn, moving medially as the RA is entered. As one drops over the limbic edge, a slight movement may be seen and/or felt, indicating that the tip has entered the fossa ovalis and a safe crossing area has been reached ( Figure 7 ). The catheter/needle are withdrawn a little further and then advanced upwards to find a catch point on the atrial septum. At this point, some operators like to move to the lateral fluoroscopic position to check that the needle is indeed pointing posteriorly. If echocardiography is being used, the catheter/needle can be seen to be causing tenting distortion of the septum. With the catheter held steady, the needle is advanced. If it crosses the atrial septum, a slight “give” is often felt or a slight movement seen. The catheter/needle are held absolutely static with the left hand until the entry of the needle into the LA cavity has been confirmed by at least two of the following: recording of an LA pressure trace, aspiration of bright red oxygenated blood or contrast injected through the needle is seen to swirl within the LA cavity. The catheter can then be advanced, but is immediately rotated to a 3 o’clock position to avoid the posterior LA wall.
This detection of the limbic edge is found in over 90% of structurally normal hearts and is the positioning method employed in the great majority of EP cases. During the catheter/needle manipulation, many operators have the hub of the needle connected to a pressure monitoring line to allow immediate identification of the change from RA to LA. Many operators also routinely maintain a pigtail catheter in the right coronary sinus to help identify the position of the aorta. If the patient shows any tendency to coughing this should be advised against at the time of puncture.
When the secundum and primum septa are not fused, the catheter/needle may cross with no or minimal upward pressure.
When there is structural heart disease and the LA is dilated, this method frequently fails to detect the limbic edge. In this circumstance, the help of visualisation is required. The simplest form of visualisation is fluoroscopy. When the LA is enlarged it is usually visible within the cardiac silhouette and attempts can be made to find a catch-point on upward pressure within the lower half of the LA silhouette.
A further step in visualisation to achieve safe puncture has been described by Inoue et al. [2828. Inoue K, Hung JS, Chen CR, Cheng TO. Mitral stenosis: Inoue balloon catheter technique. In: Cheng TO, ed Percutaneous Balloon Valvuloplasty. New York: Igaku-Shoin; 1992:237-79. ] and Hung [2929. Hung JS. Atrial septal puncture technique in percutaneous transvenous mitral commissurotomy: mitral valvuloplasty using the Inoue balloon catheter technique. Cathet Cardiovasc Diagn. 1992;26:275-84. ]. In Inoue’s method, contrast is injected into the RA and followed through until the LA cavity has been visualised ( Figure 8A ). A horizontal line is imagined from the superior end of the tricuspid valve to the right lateral edge of the LA. From the midpoint of this line, a vertical line is imagined down to the caudal edge of the LA. The recommended puncture site is on this vertical line at a distance from the caudal LA edge of just less than the height of one vertebral body. Hung’s method uses only fluoroscopy. A pigtail catheter is placed deep within the right coronary sinus; this corresponds closely to the upper end of the tricuspid valve. A horizontal line is imagined from this point to the right lateral wall of the LA fluoroscopic silhouette. The puncture point is then chosen as with Inoue’s method ( Figure 8B ). However, regardless of where one would like to cross visually, it is essential to find a catch-point for the catheter/needle tip. The fossa ovalis, which is of oval or circular shape, usually with an area of 1.5-2.4 cm2, is composed mainly of thin fibrous tissue and is the easiest and safest part of the septum for a standard puncture. The rest of the septum is thicker and consists mainly of atrial muscle fibres, but is also capable of being crossed [3030. Babaliaros VC, Green JT, Lerakis S, Lloyd M, Block PC. Emerging applications for transseptal left heart catheterization old techniques for new procedures. J Am Coll Cardiol. 2008;51:2116-22. ]. In valve disease, the position of the fossa ovalis may alter and crossing may be successfully made outside the fossa [3131. Clugston R, Lau FY, Ruiz C. Transseptal catheterization update 1992. Cathet Cardiovasc Diagn. 1992;26:266-74. ]. When the LA is enlarged, the fossa tends to be displaced inferiorly ( Figure 9 )
Injection of contrast (e.g., 30 ml at 12 ml/second) into the RA with follow-through imaging to the LA allows the area of overlap of the two atrial cavities to be identified. In the anteroposterior position, this can be memorised in relation to the vertebral bodies. Many operators use this to identify the target area for puncture, particularly when there is distorted intracardiac anatomy ( Figure 10 ).
RIGHT ANTERIOR OBLIQUE (RAO)
The steps for this fluoroscopic position are similar to those described above, but in the 40-50° RAO view, the atria are superimposed and “en face”. The fossa is usually 1-3 cm below the tip of a pigtail catheter in the aortic root and between the pigtail and the posterior RA silhouette.
LEFT ANTERIOR OBLIQUE (LAO)
Electrophysiologists also use the left anterior oblique view. In this view, one is looking end-on to the atrial septum i.e., the opposite of the en-face view seen in the RAO position. The electrophysiologists have the advantage of having a diagnostic EP catheter in the coronary sinus to mark the caudal end of the septum as well as a pigtail catheter in the aortic sinus or a His Bundle catheter to mark the upper aspect. This view confirms when the needle curve is perpendicular to the atrial septum (see below).
LATERAL
In the lateral projection, the aortic root is first marked by a pigtail catheter deep in the aortic sinuses. The transseptal needle should then be oriented medially or slightly posterior to avoid puncturing the aorta anteriorly and the posterior wall of the RA posteriorly.
It is preferable to make the descent from the SVC in the anteroposterior projection. When descending with the catheter/needle, the operator should observe two jumps - one from the SVC to the RA and one from the RA to the fossa. On reaching the level of the aortic root marked by the pigtail catheter tip, it is advisable to move temporarily to another projection (e.g., RAO) to confirm the posterior orientation of the needle. An imaginary horizontal line is then drawn passing the aortic root to the spine. The puncture site would be 3-5 mm below that line ( Figure 11 ).
Echographic guidance of the procedure
Routine diagnostic transseptal cardiac catheterisation in the hands of experienced operators, in most cases, does not need echocardiographic guidance. However, it is a tremendous imaging tool to help operators with less experience or if it is anticipated that there might be difficulty with transseptal puncture due to either unusual anatomy or pathology of the atrial septum. It is also the only current technology that allows for a very specific site puncture, as is required in a myriad of interventional procedures, such as long-tunnel PFO closure, AF ablation, closure of mitral paravalvular leaks, LAA exclusion, edge-to-edge mitral valve repair and pulmonary vein stenting ( Figure 12 ).
It must be emphasised that the use of echocardiography in many forms can significantly improve visualisation of the atrial septum during puncture [3232. Stec S, Zaborska B, Sikora-Frac M, Krynski T, Kulakowski P. First experience with microprobe transoesophageal echocardiography in non-sedated adults undergoing atrial fibrillation ablation: feasibility study and comparison with intracardiac echocardiography. Europace. 2011;13:51-6. ]. Intracardiac echocardiography, TOE and, occasionally, TTE can all help to show the tenting of the septum before puncture. They can also help to determine the best portion of the atrial septum for puncture. The use of echocardiographic guidance enables selection of the site of the puncture within the fossa ovalis according to the expected type of procedure (e.g., anterior puncture for ablation of an accessory pathway at the mitral annulus or for ablation of ventricular tachycardia versus a lower and more posterior puncture for AF ablation). The safety of the echocardiographically guided transseptal puncture is supported by reports of success rates of 99% with few complications [3333. De Ponti R, Cappato R, Curnis A, Della Bella P, Padeletti L, Raviele A, Santini M, Salerno-Uriarte JA. Trans-septal catheterization in the electrophysiology laboratory: data from a multicenter survey spanning 12 years. J Am Coll Cardiol. 2006;47:1037-42. ]. If two LA catheters are utilised during an ablation, it has been shown that even a 1-cm difference in the location of the puncture site can make a difference in ease in manoeuvring a mapping and ablation catheter [3434. Calkins H, Brugada J, Packer DL, Cappato R, Chen SA, Crijns HJ, Damiano RJ, Jr, Davies DW, Haines DE, Haissaguerre M, Iesaka Y, Jackman W, Jais P, Kottkamp H, Kuck KH, Lindsay BD, Marchlinski FE, McCarthy PM, Mont JL, Morady F, Nademanee K, Natale A, Pappone C, Prystowsky E, Raviele A, Ruskin JN, Shemin RJ, Heart Rhythm Society, European Heart Rhythm Association, European Cardiac Arrhythmia Society, American College of Cardiology, American Heart Association, Society of Thoracic Surgeons. HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up - A report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation developed in partnership with the European Heart Rhythm Association (EHRA) and the European Cardiac Arrhythmia Society (ECAS); in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), and the Society of Thoracic Surgeons (STS) - Endorsed and approved by the governing bodies of the American College of Cardiology, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, and the Heart Rhythm Society. Europace. 2007;9:335-79. ].
Intracardiac echocardiography (ICE) is widely used in the US, as demonstrated by the fact that approximately 50% of the experts involved in the 2007 consensus statement on AF ablation routinely used ICE to facilitate the transseptal procedure and/or to guide catheter ablation [3434. Calkins H, Brugada J, Packer DL, Cappato R, Chen SA, Crijns HJ, Damiano RJ, Jr, Davies DW, Haines DE, Haissaguerre M, Iesaka Y, Jackman W, Jais P, Kottkamp H, Kuck KH, Lindsay BD, Marchlinski FE, McCarthy PM, Mont JL, Morady F, Nademanee K, Natale A, Pappone C, Prystowsky E, Raviele A, Ruskin JN, Shemin RJ, Heart Rhythm Society, European Heart Rhythm Association, European Cardiac Arrhythmia Society, American College of Cardiology, American Heart Association, Society of Thoracic Surgeons. HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up - A report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation developed in partnership with the European Heart Rhythm Association (EHRA) and the European Cardiac Arrhythmia Society (ECAS); in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), and the Society of Thoracic Surgeons (STS) - Endorsed and approved by the governing bodies of the American College of Cardiology, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, and the Heart Rhythm Society. Europace. 2007;9:335-79. ]. ICE does not require heavy sedation or general anaesthesia, as are commonly required in patients undergoing TOE. However, all ICE probes are currently mono-planar (with or without Doppler capabilities), while TOE is multi-planar and some also have three-dimensional capabilities. However, ICE catheters are expensive and have significant cost implication whereas TOE probes are reusable. TOE is generally thought to give better imaging during transseptal puncture and, most importantly, during the performance of the subsequent steps in structural interventions.
Alternatively, micro TOE probes have been developed (micro TOE S8-3t Philips Healthcare Medical Systems, Andover, Massachusetts). The tip width is 7.5 mm, which is much better tolerated than conventional probes in conscious patients. It allows two-dimensional multi-planar, colour imaging with pulsed and continuous Doppler.
Whatever the imaging technique used, it requires a good understanding and collaboration between the interventionist and the echocardiographist, as well as the use of similar definitions, to optimise the performance of the procedure.
If the transseptal puncture is guided by TOE ( Figure 13 and Figure 14 ), three two-dimensional TOE planes are sequentially used to precisely define the preferred puncture site: 1) short-axis view at the base (30-50°), which allows for anterior-posterior orientation; 2) long-axis view (bicaval) at 90-120°, which allows for superior-inferior orientation; 3) four-chamber view (0°), which is used to determine the correct height above the mitral valve, which is mandatory when performing the MitraClip and other mitral procedures.
The position of the transseptal puncture needle can be identified by a tent-like doming of the inter-atrial septum towards the LA (tenting) ( Figure 15 ). Successful crossing of the septum is confirmed by the abrupt loss of tenting.
Three-dimensional X-plane imaging can facilitate the transseptal puncture by presenting short- and long-axis views simultaneously, thus providing antero-posterior and superior-inferior orientation in a single view.
When using ICE imaging, tenting of the interatrial septum should be identified in the long-axis view and clear visualisation of the point of maximal tenting should be obtained before puncturing ( Figure 16 ). The relationship with the aortic root can be obtained by counter-clockwise rotation of the ICE catheter. Confirmation of the location of the ICE catheter in the LA can be obtained by injection of non-agitated saline or contrast during ICE imaging or the presence of a left-to-right shunt with colour Doppler.
TTE guidance is seldom used because it is difficult to perform at the same time as fluoroscopic imaging. However, it could be helpful in experienced hands.
Isolated case reports have described the feasibility of transseptal puncture on echocardiographic guidance alone, without fluoroscopy, in emergency cases. However, this approach cannot be recommended at the present time.
Other novel imaging techniques, such as direct visualisation of the atrial septum [3535. Thiagalingam A, D’Avila A, Foley L, Fox M, Rothe C, Miller D, Malchano Z, Ruskin JN, Reddy VY. Full-color direct visualization of the atrial septum to guide transseptal puncture. J Cardiovasc Electrophysiol. 2008;19:1310-5. ] using infra-red emitting catheters, have shown promise in animal models, and may also help in localising a preferred puncture site in the future ( Figure 17 ).
Alternative routes to the RA
LEFT FEMORAL VEIN
If the right femoral vein is not accessible, transseptal puncture can be achieved via the left femoral vein. Displacement of the veins may produce significant abdominal discomfort, requiring opiate. Displacement may be reduced by moving the patient’s upper body towards the right.
JUGULAR
If both femoral veins cannot be used, if the IVC is occluded or when there is azygous continuation of the IVC, it is possible to perform transseptal puncture via the SVC. Access is via the right internal jugular vein and a paediatric Brockenbrough needle or an Endrys needle set is used to cross the atrial septum. If the atrial septum is not bulging towards the RA, extra curvature may need to be given to the needle. This approach has been used for mitral balloon valvuloplasty [3636. Joseph G, George OK, Mandalay A, Sathe S. Transjugular approach to balloon mitral valvuloplasty helps overcome impediments caused by anatomical alterations. Catheter Cardiovasc Interv. 2002;57:353-62. ] and can provide a more favourable trajectory in cases requiring transcatheter closure of an anteromedial mitral paraprosthetic leak [3737. Joseph G, Thomson VS. Transjugular approach for transcatheter closure of mitral paraprosthetic leak. Catheter Cardiovasc Interv. 2009;74:971-4. ].
A new dedicated apparatus for transseptal puncture via the SVC is the LA-Crosse system (St. Jude Medical, St Paul, Minneapolis) ( Figure 18 ). The LA-Crosse system has three parts: a rhythm stabiliser sheath, a guide catheter and a flexible puncture screw. The stabiliser sheath is first placed from the right internal jugular vein and advanced inferiorly through the RA until the distal end lies in the IVC. Proximal to the stabiliser sheath tip, there is a side opening which is positioned by rotation of the stabiliser sheath so that it faces the mid-RA. A small guide catheter is then placed through the stabiliser sheath, out the side opening and advanced until its distal end is in contact with the fossa ovalis. Once the tip of the guide catheter is in position in the fossa ovalis, a flexible puncture screw is advanced through the guide catheter to its tip. Once in contact with the fossa ovalis, the puncture screw is rotated and penetrates the atrial septum. The position of the puncture screw in the LA is confirmed by LA pressure, measured through the end hole of the puncture screw. An Inoue guidewire is then advanced through the puncture screw catheter into the LA.
If access from the femoral vein/IVC is possible, but a transseptal catheter position from the SVC to the LA is advantageous (as in transcatheter repair of a medial paraprosthetic valve leak), there are alternative techniques. If an antegrade approach to the medial leak is being used, a transseptal puncture is first performed from the femoral vein in a standard fashion. Once the LA has been entered, a 0.035’’ or larger guidewire (with preformed multiple terminal large loops) is advanced through a Mullins sheath so that the loops lie in the body of the LA. The proximal end of the wire is then advanced into the iliac vein or IVC and released. Through an internal jugular vein sheath, an intravascular snare is then advanced over the free end of the guidewire in the IVC or iliac vein and, once snared, the tip is slowly withdrawn out of the internal jugular sheath. Catheters can then be advanced over the externalised proximal end of the guidewire to the LA. Alternatively, if a left ventricular transapical retrograde approach to the medial leak is chosen, the left ventricular apex is first punctured percutaneously. A sheath is then placed in the left ventricular cavity and a guidewire advanced through the paravalvular leak to the LA. Usually, better stabilisation of the wire is needed to accomplish a transcatheter repair. If so, a transseptal puncture is performed in standard fashion and a snare introduced through a Mullins sheath. The tip of the left ventricular transapical wire in the LA is snared, pulled into the RA and released. A second snaring of the wire tip is then accomplished from the internal jugular vein, and the tip of the wire is carefully externalised through the internal jugular sheath as the wire is advanced from the left ventricular apical sheath. Delivery catheters for closure devices can then be advanced either from the ventricular apex or internal jugular vein.
TRANSHEPATIC
It is also possible to reach the RA via the hepatic veins. This alternative route can be used when there is an interrupted IVC, either congenital – as in patients with atrial isomerism – or acquired, e.g., extrinsic pressure from tumours or intrinsic obstruction by thrombus, tumours or devices. It can also be used when severe spinal deformities cause marked tortuosity of the IVC, when both femoral veins are chronically occluded or when there is an absence of a right-sided SVC.
This technique should not be used if there is active peritonitis, an active coagulation disorder and in some forms of anomalous hepatic vein drainage.
Technique
The thoraco-abdominal skin area is surgically prepared and draped. The procedure is done under general anaesthesia and all procedures are guided by fluoroscopy, abdominal Doppler-ultrasound and TOE. A 22 G Chiba needle is advanced under abdominal Doppler-ultrasound guidance into the hepatic vein. Saline injected through the needle identifies microbubbles passing into the RA. Additional contrast injection under fluoroscopy will confirm the location of the needle. A 0.018” guidewire is then advanced through the needle into the RA. The needle is then exchanged for a curved 9-10 Fr sheath. A 0.032-0.035” guidewire is then advanced into the SVC, and an 8 Fr Mullins sheath is advanced through the larger transhepatic sheath. The Brockenbrough needle is then advanced and a descent from the SVC into the interatrial septum is performed, as previously described for the femoral approach, and the puncture of the septum is guided by TOE. After completing the transseptal cardiac catheterisation/intervention and anticoagulation has been reversed, the transhepatic sheath is slowly withdrawn while a diluted contrast injection through the side arm identifies, by fluoroscopy, the exit of the sheath from the hepatic vein into the hepatic parenchyma. Coils or an Amplatzer® Vascular Plug (St. Jude Medical, S. Paul, Minneapolis), are then used to seal the hepatic vein access.
Routes to the right atrium
- right femoral vein
- left femoral vein
- right internal jugular vein
- transhepatic
Challenging septa
There are a number of situations in which the nature of the atrial septum can add technical difficulty to achieving successful transseptal puncture.
Atrial septal anomalies that can cause difficulty
- resistant septum
- tender septum
- bulging septum
- giant LA
- very large RA
- atrial septal aneurysm
RESISTANT SEPTUM
The septum may prove resistant to needle puncture even at the fossa ovalis. This tough, or resistant, septum is more likely to be found if there has been a previous transseptal puncture or previous cardiac surgery [3838. Marcus GM, Ren X, Tseng ZH, Badhwar N, Lee BK, Lee RJ, Foster E, Olgin JE. Repeat transseptal catheterization after ablation for atrial fibrillation. J Cardiovasc Electrophysiol. 2007;18:55-9. ], in older patients or after thoracic radiation. Increasingly forceful forward pressure on the needle may be enough to overcome the resistance. While this is usually safe with an enlarged LA, care is needed with a normal-sized LA.
A resistant atrial septum can pose a hazard because of the extra forward pressure needed to complete atrial puncture. Even if the needle alone penetrates the septum safely, passage of the Mullins dilator and sheath over the needle may also necessitate unusual forward force. This may result in a sudden forward acceleration of the needle tip/dilator/sheath combination as the atrial septum is finally bridged. The stored energy from this forward pressure can then propel the needle, dilator and sheath quickly across the LA before the operator can respond by pulling back and LA perforation can occur. A simple trick to avoid a complication is to advance the needle alone until it just penetrates into the LA. A change in the pressure recording from the needle tip indicates passage into the LA.
Alternatives to needle puncture of the septum have been developed. The Baylis curved tip catheter uses RF energy to puncture the septum (Radiofrequency Transseptal System, Baylis Medical, Montreal, Canada) ( Figure 19 and Figure 20 ). The RF energy creates a hole in the atrial septum of equivalent size to that created by a needle. An RF catheter is placed in the dilator/sheath assembly when the foramen ovale is contacted. The catheter delivers 5 W energy for 2-5 seconds and usually perforates the atrial septum after 1-4 pulses. The advantage of the Baylis catheter is that little forward pressure is needed. Thus, the RF energy can create a hole in septa that are thick, scarred or calcified, and might even be used in those with previous surgical patching. By using the Baylis catheter in such circumstances, excess forward pressure, which could result in unsuccessful puncture or perforation of the LA free wall secondary to catheter momentum after puncturing the septum, is avoided [3939. Sherman W, Lee P, Hartley A, Love B. Transatrial septal catheterization using a new radiofrequency probe. Catheter Cardiovasc Interv. 2005;66:14-7. , 4040. Capulzini L, Paparella G, Sorgente A, de Asmundis C, Chierchia GB, Sarkozy A, Muller-Burri A, Yazaki Y, Roos M, Brugada P. Feasibility, safety, and outcome of a challenging transseptal puncture facilitated by radiofrequency energy delivery: a prospective single-centre study. Europace. 2010;12:662-7. ]. However, it has been shown that RF energy can also be utilised in a simpler way via the Brockenbrough needle by using a standard electrosurgical cautery generator. Brief pulses of RF energy are applied to the hub of the transseptal needle [4141. McWilliams MJ, Tchou P. The use of a standard radiofrequency energy delivery system to facilitate transseptal puncture. J Cardiovasc Electrophysiol. 2009;20:238-40. , 4242. Smelley MP, Shah DP, Weisberg I, Kim SS, Lin AC, Beshai JF, Burke MC, Knight BP. Initial experience using a radiofrequency powered transseptal needle. J Cardiovasc Electrophysiol. 2010;21:423-7. ] either by direct contact or via a double crocodile clip connector wire. This has been found to be a very effective way of overcoming a resistant septum without the use of excessive force, which improves the safety of the procedure and also eases the performance of the transseptal puncture at a desired site for structural interventions
Just as RF catheters can be used to perforate/puncture the atrial septum, so excimer laser catheters (0.9-mm CLiRpath X-80, Spectranetics Inc., Colorado Springs, Colorado) [4343. Bommer WJ, Lee G, Riemenschneider TA, Ikeda RM, Rebeck K, Stobbe D, Ogata C, Theis JH, Reis RL, Mason DT. Laser atrial septostomy. Am Heart J. 1983;106:1152-6. , 4444. Galal O, Weber HP, Enders S, al Watban F, ElSayet RM, Duran C. Transcatheter laser atrial septostomy in rabbits. Int J Cardiol. 1993;42:31-5. , 4545. Elagha AA, Kim AH, Kocaturk O, Lederman RJ. Blunt atrial transseptal puncture using excimer laser in swine. Catheter Cardiovasc Interv. 2007;70:585-90. ] can also accomplish puncture. The laser catheter is slightly larger than the inner lumen of a standard Mullins sheath and dilator. Thus, a modified Mullins sheath and dilator (inner lumen compatible with a 0.038” wire) is used, through which the laser catheter is introduced. Excimer laser energy can puncture the septum after a brief (2-5 second) burst of laser energy. The laser catheter also requires less force to cross the septum. Once the septum has been crossed with the catheter, it can serve as a rail over which the Mullins sheath and dilator can be advanced. Data from animal studies are promising [4444. Galal O, Weber HP, Enders S, al Watban F, ElSayet RM, Duran C. Transcatheter laser atrial septostomy in rabbits. Int J Cardiol. 1993;42:31-5. , 4545. Elagha AA, Kim AH, Kocaturk O, Lederman RJ. Blunt atrial transseptal puncture using excimer laser in swine. Catheter Cardiovasc Interv. 2007;70:585-90. ]. The technology can be used with current deflectable guiding catheters (Morph catheter, Biocardia Inc., San Francisco, California and Naviport® catheter, Cardima, Fremont, California) [3030. Babaliaros VC, Green JT, Lerakis S, Lloyd M, Block PC. Emerging applications for transseptal left heart catheterization old techniques for new procedures. J Am Coll Cardiol. 2008;51:2116-22. , 4545. Elagha AA, Kim AH, Kocaturk O, Lederman RJ. Blunt atrial transseptal puncture using excimer laser in swine. Catheter Cardiovasc Interv. 2007;70:585-90. ].
Another new concept for overcoming a resistant septum is the SafeSept™ wire (Pressure Products, San Pedro, California). The 0.014” wire is advanced through the needle lumen. It is designed with a very sharp tip that can penetrate the septum more easily than the needle bevel. As soon as this wire enters the LA it takes up a J-shape to avoid touching the posterior LA wall [4646. Wadehra V, Chow AWC. Initial clinical experience of transseptal punctures performed using the SafeSept transseptal guidewire. Eplabdigestcom. 2009;9:20-1. , 4747. Wieczorek M, Hoeltgen R, Akin E, Salili AR. Use of a novel needle wire in patients undergoing transseptal puncture associated with severe septal tenting. J Interv Card Electrophysiol. 2010;27:9-13. ].
It should be stressed that these additional techniques should only be used when the location of the transseptal catheter is precisely shown by “tenting” imaged by ICE or TOE.
If the needle can cross, but not the catheter, it may be useful to introduce an exchange angioplasty 0.014 guidewire into the needle up to the left superior pulmonary vein and use it as support for both the needle and the catheter. As an alternative to this technique, rather than trying to advance the dilator and sheath over the needle, a 0.014” angioplasty guidewire can instead be threaded through the transseptal needle and looped into the LA. Passage of the sheath and dilator will then be over the looped guidewire, avoiding rapid transit to the opposite side of the LA [4848. Hildick-Smith D, McCready J, de Giovanni J. Transseptal puncture: use of an angioplasty guidewire for enhanced safety. Catheter Cardiovasc Interv. 2007;69:519-21. ].
Finally, one should keep in mind that in case of a resistant septum, it may be necessary to redo the puncture at another site, as the first attempt might be in the muscular part of the septum rather than in the fossa.
During mitral valvuloplasty, the relatively blunt-nosed Inoue balloon catheter may fail to cross the septum despite very firm pressure. The puncture point can be slightly enlarged by dilating the crossing point with a coronary or peripheral (8 mm) balloon.
Alternatives to simple needle/catheter puncture
- Baylis RF catheter
- Electrosurgical cautery generator connected to needle
- Eximer laser
- SafeSept™ wire
- balloon dilatation
TENDER SEPTUM
If asked, patients will not infrequently report a mild feeling of discomfort when puncture occurs. Very occasionally, however, a patient will immediately declare major discomfort with even modest pressure on the septum. This tender septum can usually be dealt with by use of intravenous opiate but, rarely, the tenderness is so exquisite that general anaesthesia is required.
BULGING SEPTUM
When LA pressure is very high, as it may be with severe mitral stenosis, there may be a markedly bulging septum towards the RA cavity. As a result, when the catheter/needle descends from the SVC it can repeatedly slip medially or laterally because of the bulge. Forceful torquing of the needle back onto the middle of the septum bulge usually allows successful entry to the LA.
GIANT LEFT ATRIUM
A giant LA might be thought to make transseptal puncture easier, but the opposite is often the case. It can be very difficult to find a catch point on the septum by the catheter or needle tip. Often, an unusually low, but not too posterior, position on the septum has to be used ( Figure 21 ).
It should be stressed that a too-posterior puncture, outside the borders of the fossa ovalis, should not be used in order to avoid a perforation into the pericardial space between the two atria. In such cases, the convexity of the septum due to LA enlargement may cause catheter slippage and, thus, may impede adequate contact with the septum.
VERY LARGE RA
A very large RA can make it difficult for the needle curve to reach the septum. In such cases, it is useful to slightly bend the needle at 10 cm from the tip to facilitate contact with the septum.
ATRIAL SEPTAL ANEURYSM
An atrial septal aneurysm directed into the RA cavity may be seen on preprocedural TTE. Crossing may be surprisingly easy as there is a higher incidence of associated PFO [4949. Lau KW, Ding ZP, Johan A. Percutaneous transseptal mitral valvuloplasty in the presence of atrial septal aneurysm. Cathet Cardiovasc Diagn. 1994;31:337-40. , 5050. Rittoo D, Sutherland GR, Shaw TR. Transseptal mitral balloon valvotomy in patients with atrial septal aneurysms. Cardiology. 1997;88:300-4. ] ( Figure 22 ). However, if there is resistance, the operator has to be cautious not to puncture the posterior LA wall when pressure causes the aneurysm to prolapse into the LA. When marked tenting of the septum is suspected, the posterior LA wall can be protected using a sharp Nitinol J-tipped SafeSept™ wire [4646. Wadehra V, Chow AWC. Initial clinical experience of transseptal punctures performed using the SafeSept transseptal guidewire. Eplabdigestcom. 2009;9:20-1. , 4747. Wieczorek M, Hoeltgen R, Akin E, Salili AR. Use of a novel needle wire in patients undergoing transseptal puncture associated with severe septal tenting. J Interv Card Electrophysiol. 2010;27:9-13. ] or by advancing an angioplasty wire through the needle [4848. Hildick-Smith D, McCready J, de Giovanni J. Transseptal puncture: use of an angioplasty guidewire for enhanced safety. Catheter Cardiovasc Interv. 2007;69:519-21. ].
In general, when faced with a difficult septum, several passes down the septum may be required. As an alternative to repeated exchanges between needle and guidewire to regain access to the SVC, the “anterior staircase” manoeuvre can be used [5151. Shaw TR. Anterior staircase manoeuvre for atrial transseptal puncture. Br Heart J. 1994;71:297-301. ] ( Figure 23 ). When the catheter/needle reach the inferior portion of the LA, they are rotated to have the curve pointing to 12 o’clock. The catheter/needle are then advanced to the top of the LA while moving the tip continually from side to side to confirm no snagging. As the IVC enters the RA posteriorly there is space within the RA cavity to accommodate the curve ( Figure 24 ). The catheter/needle are then rotated again to a posterior position and drawn down the septum.
If the needle achieves a catch-point but does not enter the LA cavity, some operators elect to inject a very small volume of contrast through the needle. It is said that if there is a vertically aligned stain of contrast then the position is too high and if horizontally aligned, the position is too low.
If achieving successful puncture is causing delay, the needle should be withdrawn every 4-6 minutes and the catheter back-flushed to remove any thrombus which can develop on the needle. If the Mullins sheath remains in the LA after catheter/needle withdrawal, it also needs a very vigorous flush.
Special situations
CHILDREN
For children, the most common indication for a transseptal puncture is a balloon mitral valvuloplasty procedure, particularly in developing countries [5252. Gamra H, Betbout F, Ben Hamda K, Addad F, Maatouk F, Dridi Z, Hammami S, Abdellaoui M, Boughanmi H, Hendiri T, Ben Farhat M. Balloon mitral commissurotomy in juvenile rheumatic mitral stenosis: a ten-year clinical and echocardiographic actuarial results. Eur Heart J. 2003;24:1349-56. ]. The septum is usually easy to cross but, in some cases, a fibrous and thick septum can be encountered. In these cases, care should be taken to avoid a jump of the needle from the RA to the LA, which can cause damage to the atrial wall resulting in tamponade.
PREGNANCY
Any procedure involving ionising radiation should be avoided during the first trimester whenever possible. The transseptal puncture should be performed in the usual way using the normal landmarks. The catheter/needle usually passes easily under the gravid uterus. However, in order to minimise the risk of foetal radiation, the patient’s abdomen should be shielded by a lead apron placed between the patient and the direction of the X-ray beam. For the same reason, the use of fluoroscopy should be kept to a minimum and cineangiography avoided. However, patient safety should never be compromised by excessive minimisation of the technique and general anaesthesia is useful in this setting to allow for TOE guidance. Transseptal catheterisation is performed during pregnancy mainly for a percutaneous balloon mitral valvuloplasty procedure. The transseptal puncture and balloon dilatation do not need much fluoroscopy time and studies have shown no deleterious radiation side effects in the babies after these procedures [5353. Gamra H, Ben-Farhat M, Betbout F, Addad F, Ben-Rejeb R, Dridi Z, Khedher S, Ben-Hamda K, Maatouk F, Maaoui S. Long term outcome of balloon mitral commissurotomy during pregnancy: a prospective physical and mental evaluation of babies. EuroIntervention. 2006;2:302-9. ]. In some cases, the patient needs to be in a 45° lateral position to prevent the pressure of the uterus reducing IVC flow and aggravating hypotension. This nonstandard position needs to be taken into account when controlling the angulation of the needle; however, such a position should be avoided if possible.
DEXTROCARDIA
Dextrocardia is a rare condition found in about 1 in 12,000 of the general population. Almost one-third of these persons have situs inversus [5454. Bohun CM, Potts JE, Casey BM, Sandor GG. A population-based study of cardiac malformations and outcomes associated with dextrocardia. Am J Cardiol. 2007;100:305-9. ]. When dextrocardia is not associated with situs inversus, the heart is just located in the right side of the thorax. In that case, the transseptal puncture is performed as in the normal cases with the same SVC descent and intracardiac landmarks. However, when it is associated with situs inversus, the major visceral organs including the heart are mirrored from their normal positions. The transseptal puncture is, in that case, associated with marked technical difficulties and a high risk of cardiac perforation. There are two suggested ways to deal with the transseptal puncture in that setting, either to invert the image of the fluoroscopy screen but keep thinking you are manipulating in the opposite direction to usual, or keep the image as it is but concentrate with the help of a co-operator. It may be preferable to use the left femoral vein ( Figure 25 ).
Technical aspects according to subsequent interventional procedure
TRANSSEPTAL CATHETERISATION FOR ELECTROPHYSIOLOGY PROCEDURES
Interventional electrophysiologists have used transseptal puncture since the 1980s as an alternative or complementary approach to the retro-aortic route to ablate left-sided accessory pathways. However, the spread of the technique in the EP lab has followed the development of LA ablation to treat AF.
The techniques of transseptal puncture have similarities whether used in the EP lab or in the haemodynamic or structural intervention lab, but some specific features deserve to be mentioned [2525. Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA, Crijns HJ, Damiano RJ, Jr., Davies DW, DiMarco J, Edgerton J, Ellenbogen K, Ezekowitz MD, Haines DE, Haissaguerre M, Hindricks G, Iesaka Y, Jackman W, Jalife J, Jais P, Kalman J, Keane D, Kim YH, Kirchhof P, Klein G, Kottkamp H, Kumagai K, Lindsay BD, Mansour M, Marchlinski FE, McCarthy PM, Mont JL, Morady F, Nademanee K, Nakagawa H, Natale A, Nattel S, Packer DL, Pappone C, Prystowsky E, Raviele A, Reddy V, Ruskin JN, Shemin RJ, Tsao HM, Wilber D. 2012 HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Europace. 2012;14:528-606. , 3333. De Ponti R, Cappato R, Curnis A, Della Bella P, Padeletti L, Raviele A, Santini M, Salerno-Uriarte JA. Trans-septal catheterization in the electrophysiology laboratory: data from a multicenter survey spanning 12 years. J Am Coll Cardiol. 2006;47:1037-42. , 3434. Calkins H, Brugada J, Packer DL, Cappato R, Chen SA, Crijns HJ, Damiano RJ, Jr, Davies DW, Haines DE, Haissaguerre M, Iesaka Y, Jackman W, Jais P, Kottkamp H, Kuck KH, Lindsay BD, Marchlinski FE, McCarthy PM, Mont JL, Morady F, Nademanee K, Natale A, Pappone C, Prystowsky E, Raviele A, Ruskin JN, Shemin RJ, Heart Rhythm Society, European Heart Rhythm Association, European Cardiac Arrhythmia Society, American College of Cardiology, American Heart Association, Society of Thoracic Surgeons. HRS/EHRA/ECAS expert consensus statement on catheter and surgical ablation of atrial fibrillation: recommendations for personnel, policy, procedures and follow-up - A report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation developed in partnership with the European Heart Rhythm Association (EHRA) and the European Cardiac Arrhythmia Society (ECAS); in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), and the Society of Thoracic Surgeons (STS) - Endorsed and approved by the governing bodies of the American College of Cardiology, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, and the Heart Rhythm Society. Europace. 2007;9:335-79. , 3838. Marcus GM, Ren X, Tseng ZH, Badhwar N, Lee BK, Lee RJ, Foster E, Olgin JE. Repeat transseptal catheterization after ablation for atrial fibrillation. J Cardiovasc Electrophysiol. 2007;18:55-9. , 5555. Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Quiniou G, Garrigue S, Le Mouroux A, Le Metayer P, Clementy J. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339:659-66. , 5656. Fagundes RL, Mantica M, De Luca L, Forleo G, Pappalardo A, Avella A, Fraticelli A, Dello Russo A, Casella M, Pelargonio G, Tondo C. Safety of single transseptal puncture for ablation of atrial fibrillation: retrospective study from a large cohort of patients. J Cardiovasc Electrophysiol. 2007;18:1277-81. , 5757. Michowitz Y, Rahkovich M, Oral H, Zado ES, Tilz R, John S, Denis A, Di Biase L, Winkle RA, Mikhaylov EN, Ruskin JN, Yao Y, Josephson ME, Tanner H, Miller JM, Champagne J, Della Bella P, Kumagai K, Defaye P, Luria D, Lebedev DS, Natale A, Jais P, Hindricks G, Kuck KH, Marchlinski FE, Morady F, Belhassen B. Effects of sex on the incidence of cardiac tamponade after catheter ablation of atrial fibrillation: results from a worldwide survey in 34 943 atrial fibrillation ablation procedures. Circ Arrhythm Electrophysiol. 2014;7:274-80. , 5858. Hsu JC, Badhwar N, Gerstenfeld EP, Lee RJ, Mandyam MC, Dewland TA, Imburgia KE, Hoffmayer KS, Vedantham V, Lee BK, Tseng ZH, Scheinman MM, Olgin JE, Marcus GM. Randomized trial of conventional transseptal needle versus radiofrequency energy needle puncture for left atrial access (the TRAVERSE-LA study). J Am Heart Assoc. 2013;2:e000428. ].
The main procedure categories are:
- ablation of left sided accessory pathways
- ablation of focal left atrial arrhythmias, including atrial fibrillation
- ablation of left ventricular tachycardia.
In addition, transseptal catheterisation is occasionally used to enable endocardial placement of a left ventricular pacing lead for patients requiring cardiac resynchronisation therapy in whom left ventricular lead placement cannot be satisfactorily achieved via the coronary sinus.
Specific features of transseptal puncture in the EP lab include the double transseptal technique. In most cases, more than one catheter is used for LA ablation. This is done using either a double transseptal puncture or a single puncture. In the former, a guidewire is placed in the left superior pulmonary vein through the first sheath and dilator, which are then pulled back into the RA. Next, the ablation catheter (through a second sheath) is positioned (under fluoroscopy and/or TEE or ICE) in the fossa ovalis and pushed into the LA following the guidewire direction. Finally, the first sheath and dilator are pushed over the wire into the LA ( Figure 26 ). An alternative method for the double transseptal technique with a single puncture has also been described [5959. Fisher WG, Ro AS. Trans-septal catheterization. In: Huang SKS, Wood MA, eds Catheter ablation of cardiac arrhythmias: Saunders. 2006:635-48. ].
Technical considerations during EP procedures
Placement of diagnostic EP catheters prior to transseptal puncture can provide helpful anatomical information to the operator. A quadripolar catheter placed in a position where a His bundle electrogram is recorded will identify the site of the inferior aspect of the non-coronary aortic cusp. A multipolar catheter placed in the coronary sinus will mark the orientation of the atrioventricular groove and together, these catheters provide the operator with an index of cardiac rotation. A LAO fluoroscopic view can be adjusted so that the bundle catheter is viewed end-on ( Figure 27 ). This will approximate the view along the axis of the interatrial septum. The transseptal sheath and needle can then be correctly orientated perpendicular to the septum prior to puncture. This view is also helpful in mapping left-sided accessory pathways, in which cases the coronary sinus catheter circumscribes the posterior and lateral mitral annulus. This is used as a reference for positioning the mapping catheter around the “clockface” of the mitral annulus ( Figure 28 ). The RAO view can be used to confirm the anteroposterior position of the sheath in relation to the aortic root and atrioventricular groove. Operators should be mindful of the increased radiation backscatter associated with the LAO view. In some centres, ICE is used to guide transseptal puncture and is helpful for the early identification of pericardial effusion and, in some cases, to guide the ablation procedure itself ( Figure 29 ).
Ablation of left-sided accessory pathways
Approximately 70% of accessory pathways have a left-sided location and span the mitral annulus.
Once a left-sided pathway has been identified, two approaches may be used. The ablation catheter can be guided to the mitral annulus retrogradely via the arterial circulation from the femoral artery, or it can be delivered to the mitral annulus via a transseptal sheath. The retrograde approach can be technically challenging because of the difficulty in steering the catheter as it traverses the aortic arch and is retroflexed towards the mitral annulus. Ablation catheters are quite rigid in build and have the potential to plug or injure a coronary artery, or to cause cerebral embolism. Catheter placement can also be limited by peripheral vascular disease or aortic aneurysm, although these pathologies are uncommon in most affected patients who present in early adulthood with their arrhythmias.
The transseptal approach is advantageous for ablation of left-sided accessory pathways because the catheter is naturally directed toward the lateral mitral annulus after passage through the intra-atrial septum. Puncture is normally straightforward because most patients have no associated structural heart disease and therefore normal anatomy. A Mullins transseptal sheath can be used for the initial puncture, but better support is achieved if a dedicated support sheath is used. Pre-shaped sheaths are available that allow access to different positions on the mitral annulus, providing catheter stability which is essential to deliver an effective lesion to the accessory pathway. Left posteroseptal and paraseptal pathways are the most difficult to access as the catheter has to be delivered anterior to the puncture site. This is achieved either by firm anticlockwise rotation of a short-nosed transseptal sheath or by looping the catheter all the way around the mitral annulus, where a dedicated support sheath is often needed for support.
Ablation of focal LA arrhythmias and AF
Atrial tachycardias are usually focal in origin, but can be macroreentrant (i.e., LA flutter). LA tachycardia may originate from any site in that chamber, but the antra of the pulmonary veins, the LAA and the mitral annulus are the most common sites. Pulmonary vein foci are also the most common initiators and drivers for AF. Pulmonary vein isolation techniques are used, either alone or in combination with linear ablation and focal LA ablation, to prevent AF. The two most commonly used approaches are segmental pulmonary vein isolation and circumferential ablation, where the left- and right-sided veins are encircled by a continuous ablation lesion set to achieve isolation.
Pulmonary vein anatomy is highly variable between individual patients in terms of vein size, orientation and number. There is corresponding variability in difficulty achieving proper contact between catheter and vein antrum during the ablation procedure. LA ablation procedures may involve placement of two catheters into the left heart – one reference catheter and one ablation catheter. During ablation for AF, a circular multi-electrode catheter is normally placed in the pulmonary vein ostium to allow identification of conducting tissue and to verify vein isolation during ablation. A double transseptal puncture technique is normally employed, using two separate but adjacent punctures. While it is possible to pass two transseptal sheaths through a single puncture hole using a double guidewire exchange technique, sheath manipulation is often constrained by immediate proximity of the adjacent sheath. Fixed curve sheaths for LA ablation have a leftward pointing tip to direct the catheter towards the posterior LA, where the pulmonary veins are situated, whereas the sheaths used for accessory pathway ablation tend to direct the catheter anteriorly towards the mitral annulus. For patients with difficult anatomies, steerable transseptal sheaths may be used (e.g., St. Jude Agilis™ and Bard Channel™ sheaths). These sheaths can be flexed and extended to provide an additional degree of freedom for catheter placement, but have the disadvantage of the larger outer diameter (11.4-13 Fr) required to accommodate the deflection mechanism.
Ablation of left ventricular tachycardia (VT)
Monomorphic VT can occur through several mechanisms. So-called “normal heart” VT can arise from the left ventricle as verapamil-sensitive fascicular VT, and from the left ventricular outflow tract. Bundle branch re-entrant VT and interfascicular VT usually occur in association with non-ischaemic dilated cardiomyopathy. All of these forms of VT are amenable to ablation using a retrograde aortic approach because septal or outflow tract tissue is readily accessible using that approach. However, in patients with VT occurring due to coronary artery disease, left ventricular scar normally forms the substrate. This can occur at any site in the left ventricle. Although not the approach of choice, transseptal catheterisation may be helpful in some cases where catheter manipulation is constrained using the retrograde approach [5959. Fisher WG, Ro AS. Trans-septal catheterization. In: Huang SKS, Wood MA, eds Catheter ablation of cardiac arrhythmias: Saunders. 2006:635-48. ].
PFO CLOSURE
Chapter 3.35
The presence of a long-tunnel PFO poses a challenge for many of the currently used devices. An alternative to trans-tunnel device placement has been described [6060. Ruiz CE, Alboliras ET, Pophal SG. The puncture technique: a new method for transcatheter closure of patent foramen ovale. Catheter Cardiovasc Interv. 2001;53:369-72. ], consisting of selective transseptal puncture of the most cephalad aspect of the septum primum at the fossa level in order to place a device that can sandwich both septum primum and secundum and effectively closing the PFO tunnel without causing major deformity or misalignment of the devices.
CIRCULATORY SUPPORT
Transseptal catheterization can also be used during percutaneous left ventricular assist device implantation.
The Tandem Heart (Cardiac Assist Technologies Inc., Pittsburgh, Pennsylvania) is a transseptal LA-to-femoral arterial assist device that provides left heart bypass designed for short-term circulatory support. The inflow transseptal cannula is a 21-Fr polyurethane catheter with a large end-hole and 14 side-holes to facilitate LA decompression.
Transseptal catheterization is also used in patients treated with veno arterial extracorporeal membrane oxygenation with persistent pulmonary oedema. In this situation, a venting canula is placed in the LA via transseptal catheterization and connected in the extracorporeal membrane oxygenation circuit using a Y connection [6161. Alkhouli M, Narins CR, Lehoux J, Knight PA, Waits B, Ling FS. Percutaneous Decompression of the Left Ventricle in Cardiogenic Shock Patients on Venoarterial Extracorporeal Membrane Oxygenation. J Card Surg. 2016;31:177-82. ].
- Echocardiography (TOE or ICE) allows safe specific-site crossing for new left heart interventions
CONGENITAL HEART DISEASE
The techniques to perform transseptal catheterisation safely in complex congenital heart disease vary considerably and depend on the structural anatomy of the underlying cardiac anomaly. The technique to enter the systemic atrium when there is drainage of the IVC into the venous atrium will very much depend on whether there is atrial (+/- visceral) situs solitus, inversus or ambiguous. The needle/sheath descent from the SVC into the venous atrium will also depend on whether this vessel is in alignment with the IVC or not. Thus, transseptal puncture in complex congenital malformations requires a good understanding of the pertinent anatomy in three dimensions in order to direct the tip of the needle towards the correct orientation. When in doubt, of course, the position of the needle when tenting the interatrial septum can be visualised by echocardiography, prior to actually advancing the needle, to grant a higher safety margin. In the presence of congenitally absent IVC and azygous continuation to the SVC, as is seen in patients with atrial isomerisms, one can opt for a transhepatic-transseptal approach, if the hepatic venous drainage into the venous atrium is anatomically favourable, or attempt a transseptal puncture from an SVC approach.
TRANSCATHETER MITRAL VALVE REPAIR OR IMPLANTATION
Chapter 3.30
The most common mitral valve repair technique used today is the edge-to-edge technique using the MitraClip. The transseptal puncture is performed under echo guidance, which is subsequently necessary for the performance of the procedure [6262. Wunderlich NC, Siegel RJ. Peri-interventional echo assessment for the MitraClip procedure. Eur Heart J Cardiovasc Imaging. 2013;14:935-49. ]. The determination of the optimal puncture site is of major importance for a MitraClip procedure. The puncture must be performed in the superior-posterior part of the fossa ovalis and at an adequate distance from the mitral valve ( Figure 12 ). The optimal height above the mitral valve differs for primary and secondary mitral regurgitation. In cases with primary mitral regurgitation, the puncture site should be 4-5 cm above the mitral annulus, thus providing enough space to adequately manoeuvre the delivery system within the LA. In patients with secondary mitral regurgitation, important valve tethering most often results in a shift in the position of the line of coaptation to below the mitral annulus. Subsequently, transseptal puncture needs to be lower, approximately 3.5 cm above the annular plane or 4-4.5 cm above the coaptation of both leaflets in order to be able to advance the catheter more deeply into the LA.
The bicaval TOE view allows visualisation of the “height” of puncture in the septum, while the short-axis view best shows how far “posterior” the puncture is to be made. Lastly, the four-chamber view shows the distance from the puncture site to the point of mitral valve coaptation ( Figure 13). An ideal puncture should be made so that the distance to the line of coaptation in the four-chamber view is 3.5-4 cm to allow adequate space for clip manipulation and proper deployment in the mitral leaflets.
An inadequate puncture site will lead to the following complications: aortic hugging (if the puncture is too anterior, e.g., through a PFO); inability to cross the mitral valve in a too-high puncture; inability to pull back the clip and tether the leaflets after a too-low puncture; and risk of perforation if the puncture is too posterior.
The stability of the position of the needle should be carefully checked before pushing the sheath over the needle. For this purpose, the use of RF energy could be a useful adjunct by avoiding the potential slippage of the needle while applying force to cross the septum.
Experience of other mitral interventions is growing, e.g. “valve-in-a-valve” ( Figure 30) or “valve-in-a-ring” or direct annuloplasty [1313. Bouleti C, Fassa AA, Himbert D, Brochet E, Ducrocq G, Nejjari M, Ghodbane W, Depoix JP, Nataf P, Vahanian A. Transfemoral implantation of transcatheter heart valves after deterioration of mitral bioprosthesis or previous ring annuloplasty. JACC Cardiovasc Interv. 2015;8:83-91. ], [6363. Guerrero M, Urena M, Himbert D, Wang DD, Eleid M, Kodali S, George I, Chakravarty T, Mathur M, Holzhey D, Pershad A, Fang HK, O’Hair D, Jones N, Mahadevan VS, Dumonteil N, Rodes-Cabau J, Piazza N, Ferrari E, Ciaburri D, Nejjari M, DeLago A, Sorajja P, Zahr F, Rajagopal V, Whisenant B, Shah PB, Sinning JM, Witkowski A, Eltchaninoff H, Dvir D, Martin B, Attizzani GF, Gaia D, Nunes NSV, Fassa AA, Kerendi F, Pavlides G, Iyer V, Kaddissi G, Witzke C, Wudel J, Mishkel G, Raybuck B, Wang C, Waksman R, Palacios I, Cribier A, Webb J, Bapat V, Reisman M, Makkar R, Leon M, Rihal C, Vahanian A, O’Neill W, Feldman T. 1-Year Outcomes of Transcatheter Mitral Valve Replacement in Patients With Severe Mitral Annular Calcification. J Am Coll Cardiol. 2018;71:1841-53. , 6464. Urena M, Brochet E, Lecomte M, Kerneis C, Carrasco JL, Ghodbane W, Abtan J, Alkhoder S, Raffoul R, Iung B, Nataf P, Vahanian A, Himbert D. Clinical and haemodynamic outcomes of balloon-expandable transcatheter mitral valve implantation: a 7-year experience. Eur Heart J. 2018;39:2679-89. , 6565. Messika-Zeitoun D, Nickenig G, Latib A, Kuck KH, Baldus S, Schueler R, La Canna G, Agricola E, Kreidel F, Huntgeburth M, Zuber M, Verta P, Grayburn P, Vahanian A, Maisano F. Transcatheter mitral valve repair for functional mitral regurgitation using the Cardioband system: 1 year outcomes. Eur Heart J. 2019;40:466-72. , 6666. Maisano F, La Canna G, Latib A, Denti P, Taramasso M, Kuck KH, Colombo A, Alfieri O, Guidotti A, Messika-Zeitoun D, Vahanian A. First-in-man transseptal implantation of a "surgical-like" mitral valve annuloplasty device for functional mitral regurgitation. JACC Cardiovasc Interv. 2014;7:1326-8. ]. There is, however, no specific recommendation concerning the transseptal technique. As a general rule, the transseptal puncture for these procedures shares most of the characteristics of that used for the MitraClip technique, i.e., a superior and posterior puncture in order to allow for sufficient manoeuvrability in the LA and crossing of the mitral valve [1313. Bouleti C, Fassa AA, Himbert D, Brochet E, Ducrocq G, Nejjari M, Ghodbane W, Depoix JP, Nataf P, Vahanian A. Transfemoral implantation of transcatheter heart valves after deterioration of mitral bioprosthesis or previous ring annuloplasty. JACC Cardiovasc Interv. 2015;8:83-91. , 6767. Urena M, Himbert D, Brochet E, Carrasco JL, Iung B, Nataf P, Vahanian A. Transseptal Transcatheter Mitral Valve Replacement Using Balloon-Expandable Transcatheter Heart Valves: A Step-by-Step Approach. JACC Cardiovasc Interv. 2017;10:1905-19. ].
MITRAL PARAVALVULAR LEAKS CLOSURE
Paravalvular leak (PVL) occurs in 5-17% of patients undergoing surgical valve replacement [6868. Hammermeister K, Sethi GK, Henderson WG, Grover FL, Oprian C, Rahimtoola SH. Outcomes 15 years after valve replacement with a mechanical versus a bioprosthetic valve: final report of the Veterans Affairs randomized trial. J Am Coll Cardiol. 2000;36:1152-8. ] and may have clinical consequences such as congestive heart failure or haemolysis. Percutaneous closure of PVLs is currently the first-line treatment of symptomatic PVLs. Some operators recommend the adaptation of the transseptal puncture according to the location of PVL [6969. Giblett JP, Rana BS, Shapiro LM, Calvert PA. Percutaneous management of paravalvular leaks. Nat Rev Cardiol. 2019:[Epub ahead of print]. ]. In this case, a high transseptal puncture is preferred for a lateral PVL (6 to 12 o’clock) and a lower puncture is preferred for a septal PVL (12 to 6 o’clock). This point is, however, a matter of debate since other groups recommend a high transseptal puncture regardless of the location of the PVL.
CLOSURE OF THE LEFT ATRIAL APPENDAGE
Chapter 3.38
The LAA is variable in its size, shape and position. Its orifice usually lies almost directly across the LA from the site of the fossa ovalis, though variability in the size and exact position of the orifice is common.
Here again, the location of the transseptal puncture is important and somewhat dependent on the particular characteristics of the device to be implanted in order to facilitate coaxial alignment and reduce the risk of complications, such as tamponade or embolization. Considering the anatomy of LAA (superior with an anterior orientation in most cases), the ideal location for transseptal puncture is most often inferior and posterior, which allows a coaxial engagement of the appendage. This has, however, to be adapted depending on patient anatomy ( Figure 12 ).
Slight rotation of the delivery sheath may be required to reach an LAA orifice that is positioned anteriorly, or replacement with a delivery sheath which has a double bend is usually successful.
PERCUTANEOUS MITRAL COMMISSUROTOMY
Chapter 3.29
The optimal position for transseptal puncture for balloon mitral valvotomy is either directly in the centre of the fossa ovalis or, preferably, slightly “low” in the fossa ( Figure 12 ). Such a puncture site allows the transseptal sheath and, ultimately, the balloon dilation catheter to follow a trajectory slightly above and across the plane of the mitral annulus. This allows the balloon dilation catheter to engage and cross the stenotic mitral valve with only a minimal bend toward the apex of the left ventricle. A “low” puncture is particularly important if the rarely used double-balloon technique is employed, though even with the Inoue balloon catheter, it facilitates crossing of the mitral valve. However, if crossing the mitral valve is not possible using this puncture location, it may be necessary to redo the transseptal puncture in a slightly higher position and more posteriorly [7070. Vahanian A, Palacios IF. Percutaneous approaches to valvular disease. Circulation. 2004;109:1572-9. ].
Complications
Complications of transseptal puncture
- atrial arrhythmias
- vasovagal reaction
- embolism
- puncture outside atrial cavities
- haemopericardium
- post-puncture atrial septal defect
Reports from various centres show that, in experienced hands, traditional transseptal puncture is a very safe technique with successful access to the LA in about 99% of cases and with serious complications in <1% [3333. De Ponti R, Cappato R, Curnis A, Della Bella P, Padeletti L, Raviele A, Santini M, Salerno-Uriarte JA. Trans-septal catheterization in the electrophysiology laboratory: data from a multicenter survey spanning 12 years. J Am Coll Cardiol. 2006;47:1037-42. ]. The support of echocardiography to confirm tenting by the needle at an appropriate part of the septum has protected less experienced operators and those using the new left heart interventions that require specific-site crossing [3030. Babaliaros VC, Green JT, Lerakis S, Lloyd M, Block PC. Emerging applications for transseptal left heart catheterization old techniques for new procedures. J Am Coll Cardiol. 2008;51:2116-22. ]. However, a number of complications can occur and may be life-threatening. Every cardiac laboratory undertaking transseptal puncture must be set up to deal with the potential complications, including instant access to TTE to confirm or exclude haemopericardium.
ATRIAL ARRHYTHMIAS
The presence of the guidewire and catheter/needle in the RA or LA can trigger an atrial tachyarrhythmia. Usually, these are self-terminating, but occasionally intravenous antiarrhythmic therapy is needed.
VASOVAGAL REACTION
As with any cardiac catheterisation, the patient may become vasovagal at any stage and require drug/fluid therapy. There are several case reports of a much more intense and treatment-resistant bradycardia/hypotension. This response has been ascribed to a Bezold-Jarisch-like reflex triggered by irritation of fibres within the atrial septum [7171. Arita T, Kubota S, Okamoto K, Kuma F, Nakasuga K, Koga H, Ito H, Maruyama T, Kaji Y, Harada M. Bezold-Jarisch-like reflex during Brockenbrough’s procedure for radiofrequency catheter ablation of focal left atrial fibrillation: report of two cases. J Interv Card Electrophysiol. 2003;8:195-202. ]. It is sometimes accompanied by transient ST elevation in the inferior leads: immediate coronary angiography has shown no abnormality and it has been postulated that this reflex has triggered coronary spasm although it is difficult to exclude the possibility of micro air-bubbles [7272. Efremidis M, Letsas KP, Xydonas S, Koutras K, Sideris A, Kardaras F. ECG findings of acute myocardial infarction and atrioventricular block during a transseptal procedure for left atrial ablation. Hellenic J Cardiol. 2008;49:284-7. ].
A very intense bradycardia and hypotension can also rarely be caused by bruising within the mediastinum after an apparently successful septal crossing. In this scenario, the catheter may have crossed outside the atria by traversing a cleft between the two enlarged atria. If this situation is suspected, it is vital not to pull back the catheter, but rather to send the patient to surgery. Immediate removal of the catheter can cause the patient to exsanguinate on the catheterisation table.
EMBOLISM
Meticulous care is required to avoid entry of air into the catheter or needle. Regular back-flushing of the catheter is needed if the puncture procedure is prolonged, as the stainless steel needle can induce thrombosis. The use of TOE/ICE has shown that instrumentation of the atria can cause small thrombi within the cavities. In patients undergoing LA ablation for AF, ICE identified thrombi in 10.3%: the thrombi were attached to a sheath or mapping catheter and most were drawn back to the RA when the catheters were withdrawn [7373. Ren JF, Marchlinski FE, Callans DJ. Left atrial thrombus associated with ablation for atrial fibrillation: identification with intracardiac echocardiography. J Am Coll Cardiol. 2004;43:1861-7. ].
PUNCTURE OUTWITH THE ATRIAL CAVITIES
If, after advancement of the catheter/needle, there is no recording of LA pressure, then there may have been perforation of the atrial wall. The risk of this developing is higher if the septum is resistant and the LA cavity small. If only the needle has perforated, it can be withdrawn safely (a situation similar to the early pre-transseptal techniques), but if the much larger catheter has perforated, then major bleeding is almost inevitable and the patient should be sent for catheter removal at open thoracic surgery. To differentiate those two circumstances, a tiny amount (0.1-0.3 ml) of contrast can be injected through the needle. If this causes staining outside the atrial cavity, then needle perforation is confirmed. The needle can then be withdrawn to just within the catheter tip while the catheter remains absolutely static. A further injection of contrast is given via the needle. If contrast swirls within the atrial cavity, the catheter has not exited the heart and can be withdrawn. If further staining is seen, the patient requires surgery for safe catheter removal [7474. Mullins CE. Cardiac catheterization in congenital heart disease: pediatric and adult. (chapter 8) Maldon, Mass: Blackwell Futura. 2006. ].
If only the needle enters the aorta, there is a general view that it can be withdrawn. If the catheter enters the aorta, the patient should be referred for thoracic surgery. If the patient is considered entirely unsuitable for surgery, there is an anecdotal report of effective catheter removal by passing a guidewire to the aorta and progressively downsizing the catheter size under echo-surveillance. Percutaneous repair of aortic puncture with an Amplatzer closure device has also been described [7575. Webber MR, Stiles MK, Pasupati S. Percutaneous repair of aortic puncture with Amplatzer closure device during attempted transseptal puncture. J Invasive Cardiol. 2013;25:E110-3. ].
HAEMOPERICARDIUM
Advancement of the catheter/needle to outside the atrial cavities can cause bleeding into the pericardium. The first clinical signs are a drop in blood pressure and a diminution of movement of the cardiac silhouette. If the haemopericardium remains small or moderate and the clinical signs are stable, then the patient can simply be closely monitored. If cardiac tamponade is threatening, then immediate echo-guided aspiration is needed: blood can be auto-transfused back to the patient. If the situation does not stabilise, referral for emergency thoracic surgery is required. In the early experience of transseptal puncture, cardiac tamponade occurred in 21 of 1,765 patients (1.2%) [7676. Braunwald E. Cooperative study on cardiac catheterization; Transseptal left heart catheterization. Circulation. 1968;37:III74-9. ]. Eighteen responded to medical measures while two required surgery; two of the patients died.
The potential dramatic consequences of this complication require an immediate access to TTE when transseptal puncture is performed.
POST-PUNCTURE ATRIAL SEPTAL DEFECT
TOE or ICE have shown that there is almost always a small left-to-right shunt visible after any septal puncture procedure. However, follow-up echo studies show that virtually all have resolved by 3 months.
Training and the use of simulators
Transseptal cardiac catheterisation is a technique that was routinely taught by many cardiology training programmes 30 years ago, but its use markedly declined as the need for haemodynamic information was being provided by alternative technologies with greater comfort and safety margins. The initiation of interventional procedures in the left cardiac chambers pioneered by balloon mitral valvuloplasty in the mid-1980s resurrected the need for transseptal catheterisation. However, the presence of a learning curve has been well described [3333. De Ponti R, Cappato R, Curnis A, Della Bella P, Padeletti L, Raviele A, Santini M, Salerno-Uriarte JA. Trans-septal catheterization in the electrophysiology laboratory: data from a multicenter survey spanning 12 years. J Am Coll Cardiol. 2006;47:1037-42. , 7777. Roelke M, Smith AJ, Palacios IF. The technique and safety of transseptal left heart catheterization: the Massachusetts General Hospital experience with 1,279 procedures. Cathet Cardiovasc Diagn. 1994;32:332-9. ]. Thus, there is a need for training courses that can teach the procedure both from the didactic and practical points of view. Such courses have recently been introduced to cater for the recently developed interventions (e.g., edge-to-edge mitral repair, LAA closure). The didactic lectures should include indications, contraindications, imaging and step-by-step techniques in the presence of normal anatomy, as well as altered chamber size and different pathologies, and how to avoid, recognise and resolve complications. Practical teaching may be obtained by performing a reasonable number of procedures with an experienced proctor. However, today, there are simulators with excellent imaging information to teach the procedure step-by-step and some of them even have reliable tactile feedback [7878. De Ponti R, Marazzi R, Ghiringhelli S, Salerno-Uriarte JA, Calkins H, Cheng A. Superiority of simulator-based training compared with conventional training methodologies in the performance of transseptal catheterization. J Am Coll Cardiol. 2011;58:359-63. ].
Personal perspective – Gregory Ducrocq / Alec Vahanian / Stuart R.D. Shaw
Transseptal puncture into the LA was a clever solution to the problem of access to the heart’s most inaccessible chamber. Its use in accurately measuring the haemodynamics of left heart valve disease improved diagnosis and the selection of patients for valve replacement. However, the technique almost died away with the emergence of two-dimensional Colour Flow Doppler echocardiography and became virtually confined to centres undertaking mitral valvuloplasty and some ablation procedures. During the last two decades, the use of transseptal puncture has risen massively due to two techniques – left heart ablation for AF and then, since the turn of the century, the new left heart interventions. This has brought refreshing new ideas and devices to the technique, including RF energy to help cross a resistant septum, new interest in the SVC approach and potential new imaging modalities. However, the biggest change has been the link-up between transseptal puncture and intra-procedure echocardiography – TOE or ICE. This also gives reassurance to inexperienced operators and to anyone dealing with very difficult distorted anatomy. With the new interventions, the search for a safe crossing point at the fossa ovalis has been replaced with a need to find a safe but site-specific crossing appropriate for the apparatus. Intra-procedure echo provides this. We think the indications for transseptal puncture will continue to expand in the future and it will be used for mitral valve implantation. It has been a rollercoaster ride for this old technique, but it is back in mainstream cardiology. Learning side-by-side with a mentor will continue to be crucial, but the new training courses and simulators will help.
Recommended bibliography
Alkhouli M, Rihal CS, Holmes DR, Jr. Transseptal Techniques for Emerging Structural Heart Interventions. JACC Cardiovasc Interv. 2016;9:2465-80.
Brockenbrough EC, Braunwald E, Ross J, Jr. Transseptal left heart catheterization. A review of 450 studies and description of an improved technic. Circulation. 1962;25:15-21.
Leon-Sit P, Callans D. Equipment for transseptal punctures. In: Thakur R, Natale A, eds. Transseptal Catheterisation and Interventions. Minneapolis: Cardiotext Publishing; 2010:55-64.
Hung JS. Atrial septal puncture technique in percutaneous transvenous mitral commissurotomy: mitral valvuloplasty using the Inoue balloon catheter technique. Cathet Cardiovasc Diagn. 1992;26:275-84.
Babaliaros VC, Green JT, Lerakis S, Lloyd M, Block PC. Emerging applications for transseptal left heart catheterization old techniques for new procedures. J Am Coll Cardiol. 2008;51:2116-22.
De Ponti R, Cappato R, Curnis A, Della Bella P, Padeletti L, Raviele A, Santini M, Salerno-Uriarte JA. Trans-septal catheterization in the electrophysiology laboratory: data from a multicenter survey spanning 12 years. J Am Coll Cardiol. 2006;47:1037-42.
Joseph G, George OK, Mandalay A, Sathe S. Transjugular approach to balloon mitral valvuloplasty helps overcome impediments caused by anatomical alterations. Catheter Cardiovasc Interv. 2002;57:353-62.
Smelley MP, Shah DP, Weisberg I, Kim SS, Lin AC, Beshai JF, Burke MC, Knight BP. Initial experience using a radiofrequency powered transseptal needle. J Cardiovasc Electrophysiol. 2010;21:423-7.


















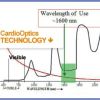

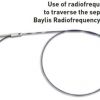




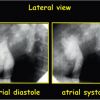

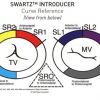

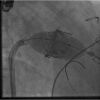

{kind=link}
{kind=link}
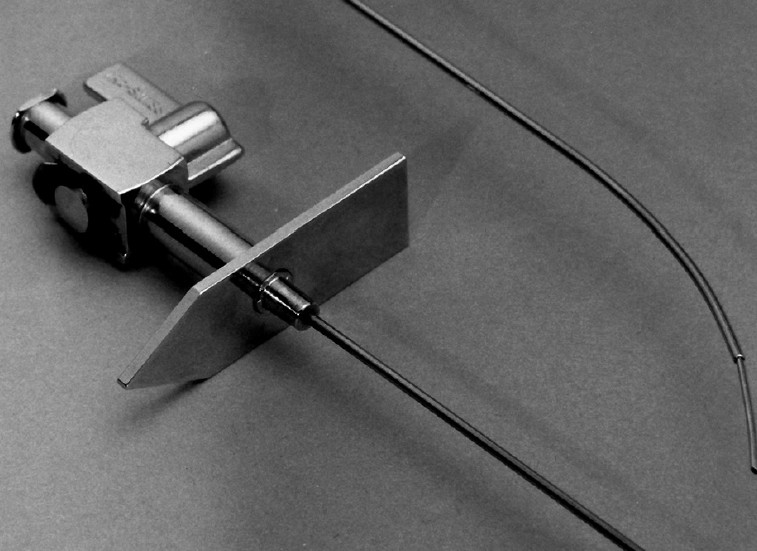{kind=link}
{kind=link}
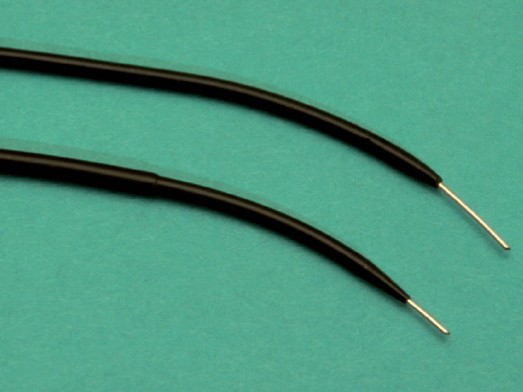{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
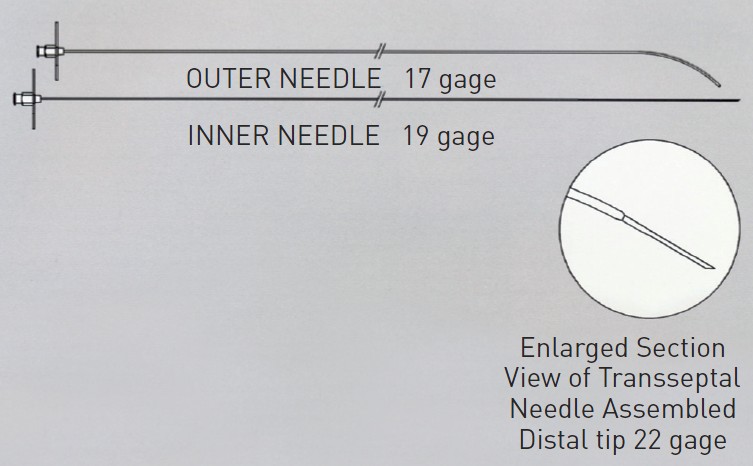{kind=link}
{kind=link}
{kind=link}
{kind=link}
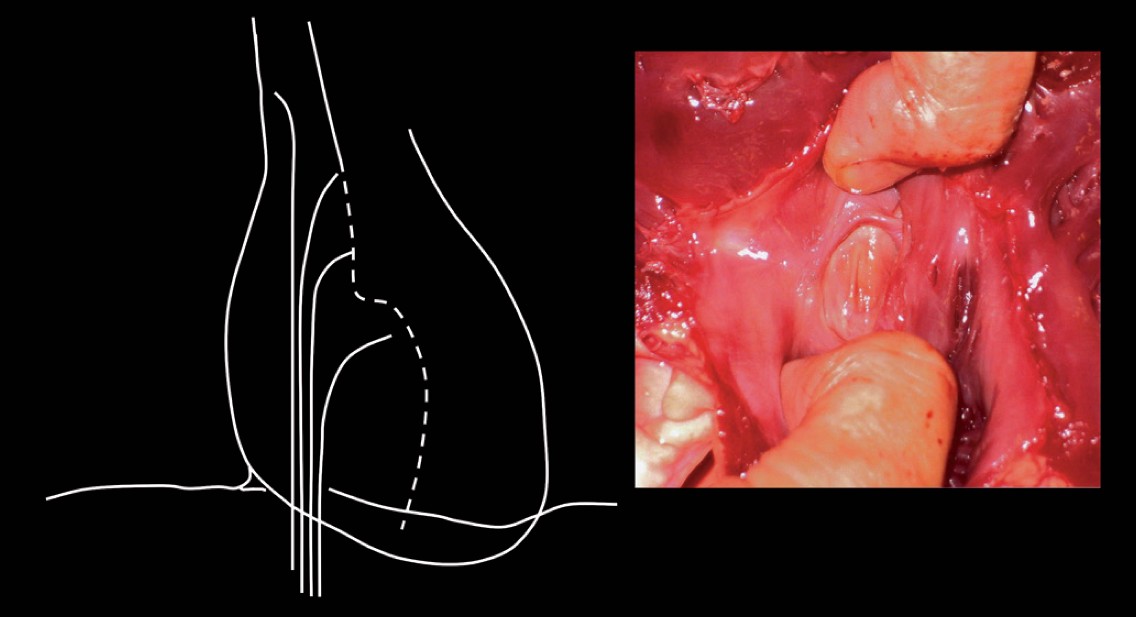{kind=link}
{kind=link}
{kind=link}
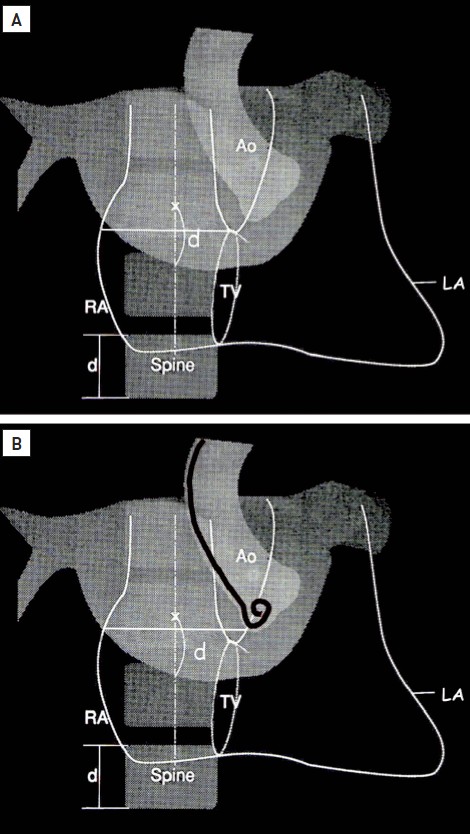{kind=link}
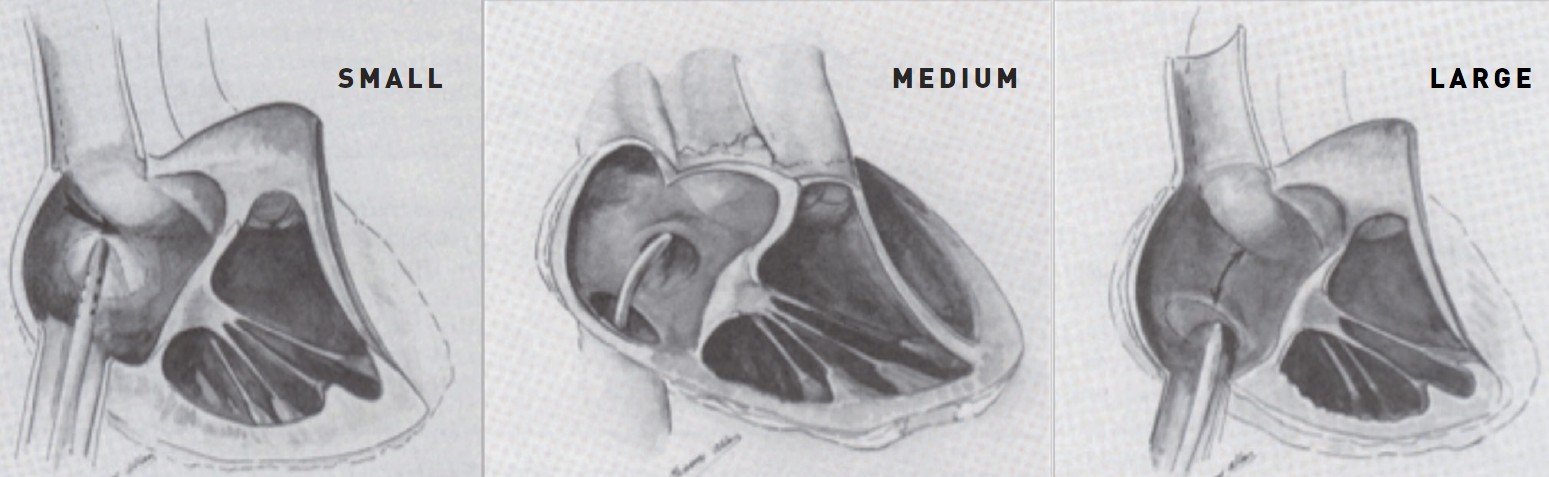{kind=link}
{kind=link}
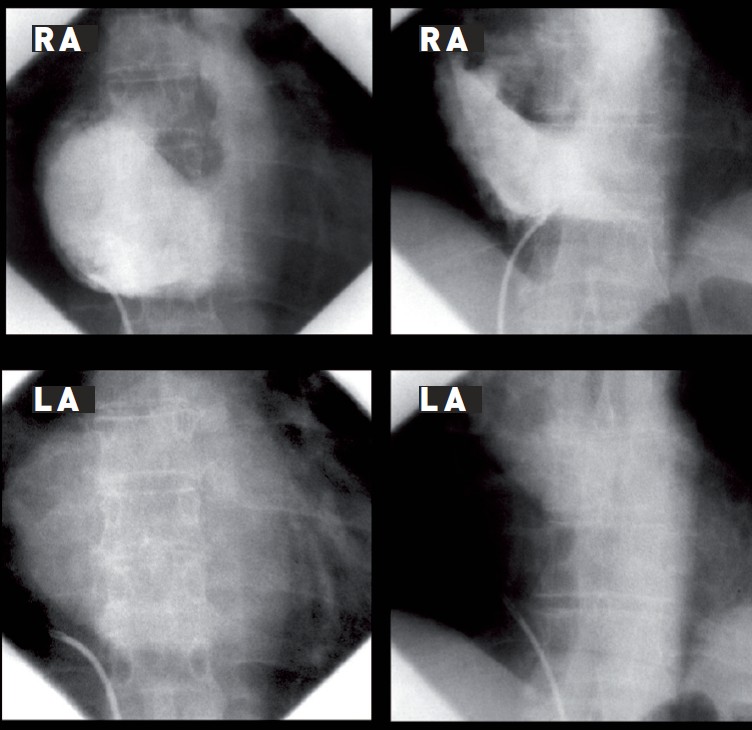{kind=link}
{kind=link}
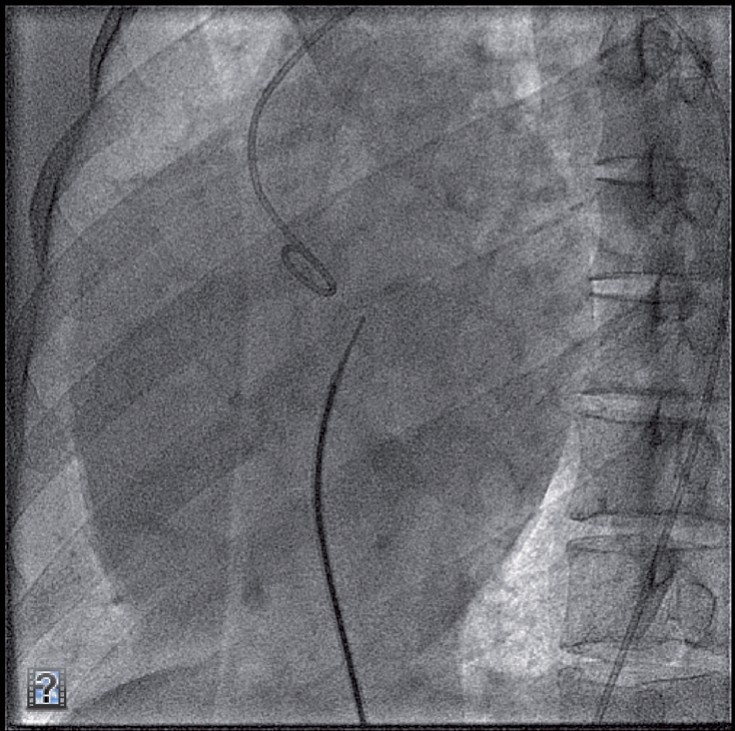{kind=link}
{kind=link}
{kind=link}
{kind=link}
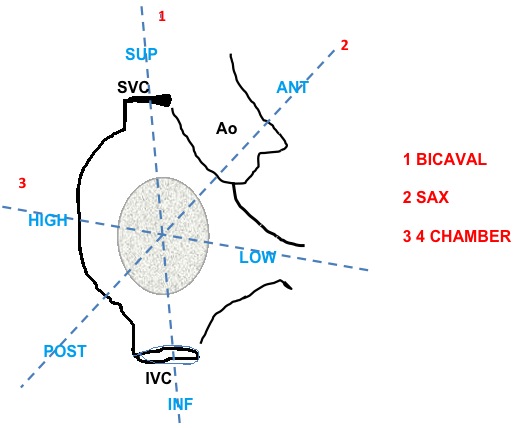{kind=link}
{kind=link}
{kind=link}
{kind=link}
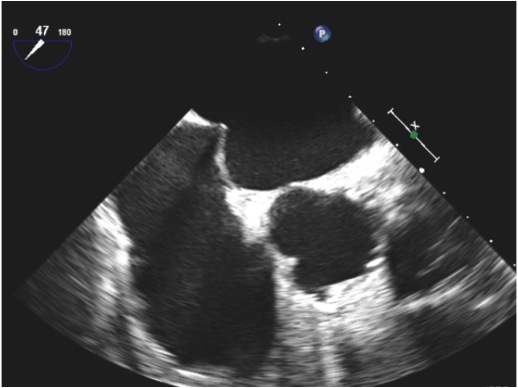{kind=link}
{kind=link}
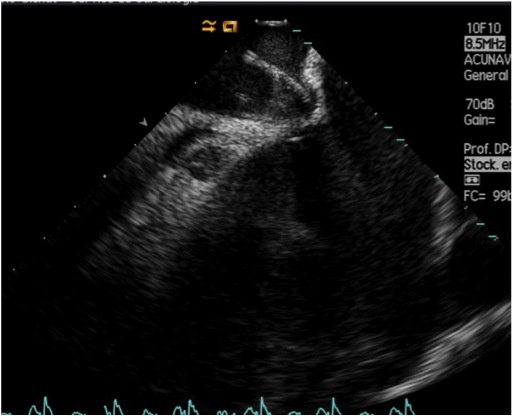{kind=link}
{kind=link}
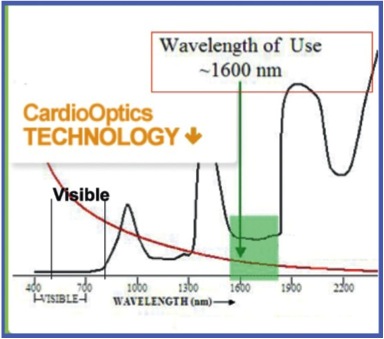{kind=link}
{kind=link}
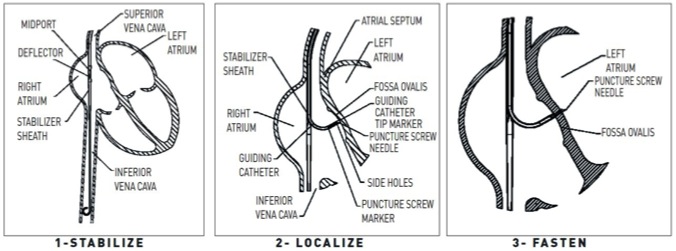{kind=link}
{kind=link}
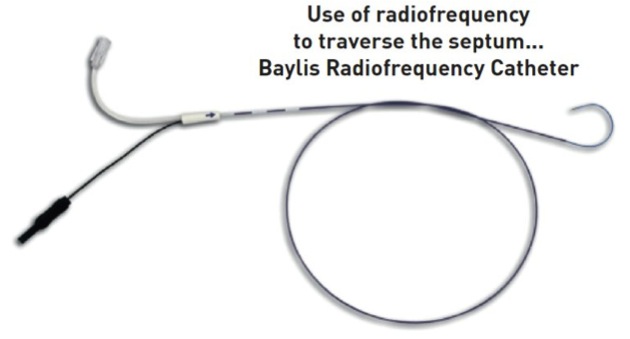{kind=link}
{kind=link}
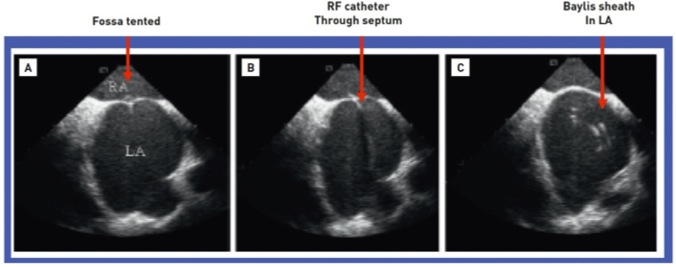{kind=link}
{kind=link}
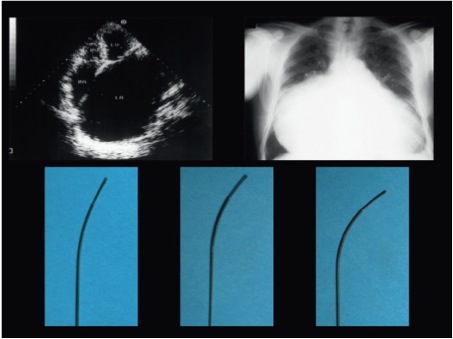{kind=link}
{kind=link}
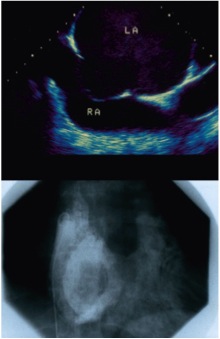{kind=link}
{kind=link}
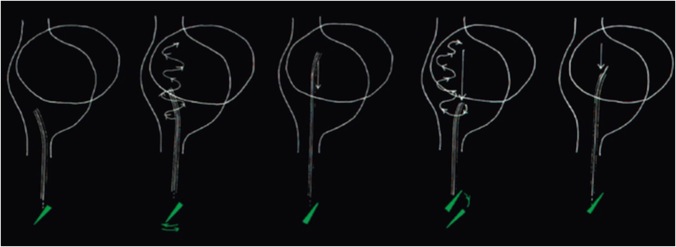{kind=link}
{kind=link}
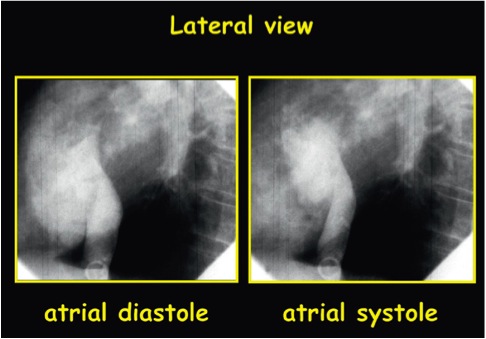{kind=link}
{kind=link}
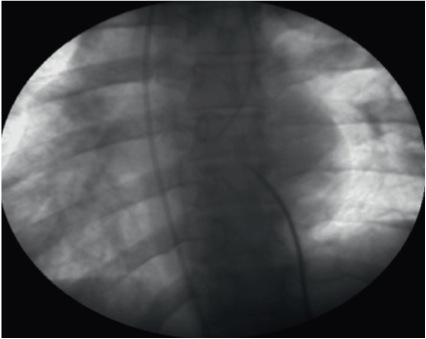{kind=link}
{kind=link}
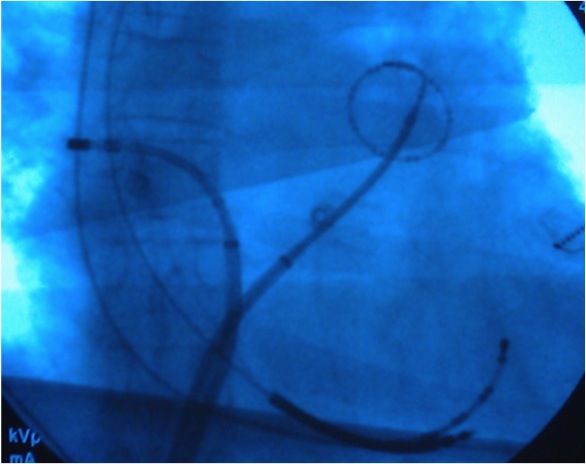{kind=link}
{kind=link}
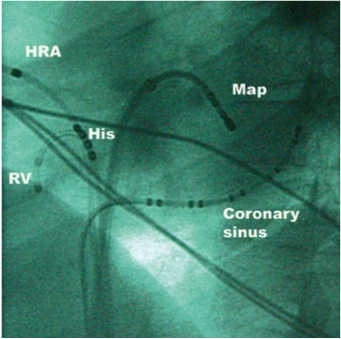{kind=link}
{kind=link}
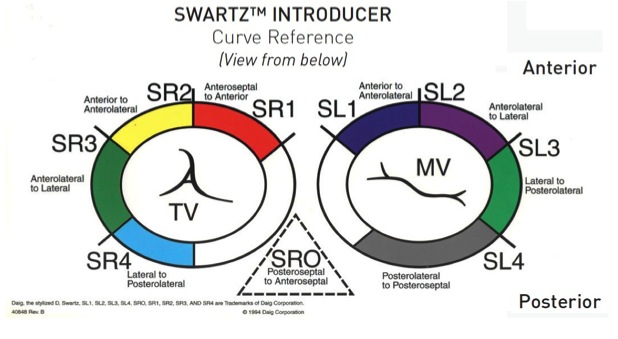{kind=link}
{kind=link}
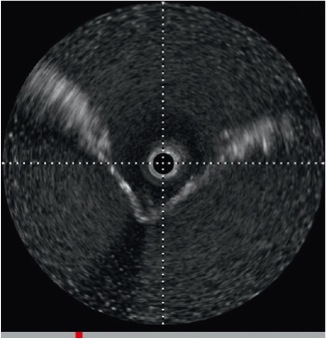{kind=link}
{kind=link}
{kind=link}
Very interesting
Congratulations!!!
fantastic review.. Congratulations
excelent chapter congratulations!!!