



Case presentation
The case was a heavily calcified proximal RCA CTO, with an ill-defined proximal cap ( Video 1), > 40 mm length of occlusion, calcified bending inside, well-defined distal cap, prior failed PCI of bilateral approach (J-CTO score of 5). There were epicardial collaterals from the distal LCX ( Video 2) in a status post-CABG, where there was a LAD occlusion with a patent LIMA graft ( Video 3), proximal disease in LCX( Video 4), and patent VG to a diseased IMD branch ( Video 5).
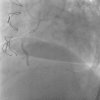
A Sion wire crossed the epicardial collateral ( Figure 1) over a Caravel microcatheter 150cm, both of which were further advanced to the proximal RCA ( Figure 2). A retrograde wire, now a Sionblack wire (Asahi Intecc, Japan), conformed a Knuckle shape, whereas an antegrade Sionblue wire (Asahi Intecc, Japan) accessed to the marginal branch ( Figure 3).
Image store of rotational fluoroscopy identified the proximity of the two gears, which later enabled a retrograde Gaia 3 to enter an Antegrade Guide of 7F AR 1.0(Retrograde wire crossing, Figure 4). An RG3 successfully obtained a wire externalization, but the tip of the Caravel was detached by forceful pulling and rotation since the wire and microcatheter was stuck within the collateral ( Figure 5).
Another Sion was advanced, and the mid-segment was dilated by a 2.0 mm balloon ( Figure 6), and the whole retrograde gears were forcefully removed from the system. SDS of DES (2.5mmx24mm) was delivered but was stuck in the calcified mid-RCA, and the stent was dislodged by way of repositioning ( Video 6).
A new Sion black successfully crossed through the deformed stent ( Video 7), followed by 1.5mm and 2.5 mm balloon dilation for deploying the stent. Additional 3.0 mm long DES deployment ( Figure 7) and post NC balloon dilation achieved a successful recanalization ( Video 8)
Heavy calcification and tortuosity remain challenging barrier for any catheter based coronary intervention. However, stepwise approach and case-based measure can find flexible solution in an unpredictable turn of the event.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}