



Case presentation
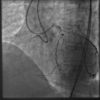
The proximal RCA CTO (including In-Stent Restenosis(occlusion): ISR), which has a blunt proximal cap, >40mm length, poor distal target, bending inside, probable interventional collaterals, and prior failed attempt (J-CTO score of 4), was approached bilaterally by 7 F Guide systems. A Gaia 3 wire punctured RCA ostial cap ( Video 1). Since the proximal CTO was hard to cross, and a distal gap present between the stent end and a distal cap ( Figure 1), a possible retrograde approach was explored by selective injection of a major septal branch, which described a connecting channel with several fuzzy tortuosities in the mid to lower septal ( Video 2).
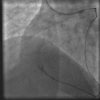
A combination of a Suoh 03 and a Caravel microcatheter 150cm (both Asahi Intecc, Japan) crossed the septal expeditiously, by an inchworm fashion over timely advanced Caravel to support ( Video 3). After septal crossing with a Caravel rotation over the wire, selective injection disclosed vaguely around the distal cap ( Figure 2).
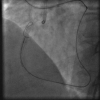
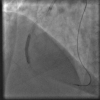
A knuckle wire of Sion black ( Figure 3) (Asahi Intecc, Japan) and Confianza Pro 12 (Asahi Intecc, Japan) successfully crossed to an Aorta, which was confirmed by touching an Antegrade JR 4.0 Guide Catheter ( Figure 4).
Guidewire Rendezvous with the Guide succeeded inside the Aorta ( Figure 5). A successful Guidewire externalization followed this by an RC3 330 cm wire (Asahi Intecc, Japan). Ballooning ( Figure 6) and IVUS were performed, and Re-implantation of DES resulted in an excellent result ( Video 4). When a retrograde angiography confirmed a significant septal hematoma, however ( Video 5), the patient did not have chest pain nor hemodynamic instability and EKG changes. Transthoracic echo failed to disclose a septal hematoma, but it was deemed necessary to control the hematoma expansion.
An attempt was made to decompress the hematoma by advancing a Sion over the Caravel into the septal. A wire was exchanged to a Ultimatebros 3g to flip the tip to the left (RV direction) ( Video 6). After more than 45 min waiting period, angiography demonstrated a decompressed septal hematoma (secondarily to a fenestration from hematoma to RV) ( Video 7) and preserved left coronary system. The clinical course was eventful, and the patient was discharged well the next day.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}