



Case presentation
The LAD CTO was found to be an ambiguous proximal take-off, 20mm length, poor distal landing zone visualized from both Right to Left and Left to left collaterals, and prior failed attempt ( Video 1, 2). After the failed attempt of proximal cap puncture using IVUS, the collateral crossing started by injecting an ipsilateral micro- tortuous epicardial collateral of the first diagonal branch ( Video 3).
Advancing a Suoh 03 over a Caravel 150cm encountered difficulty in a wire tip folding back as a knuckle shape ( Video 4), but a further pushing of the wire allowed a small knuckle tip to float through the tortuous segment of collateral to the distal LAD ( Video 5), which was confirmed by contrast injection ( Video 6).
Successful advancement of a wire and Caravel to the distal cap allowed an exchanged wire of Gaia Next 1 to cross the CTO under IVUS guidance ( Video 7), which directly visualized ( Video 8), followed by a Guidewire externalization by an RG3 after Caravel entering another Guide catheter (Ping-Pong Guide catheter).
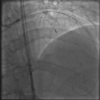
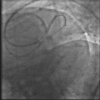
IVUS interrogation confirmed a wire tracking of the intimal and a reference vessel size ( Figure 1), and ballooning and a V-stent delivery of DES over the bifurcation ( Figure 2) led to a successful recanalization ( Video 9).
The blunt cap and steep angulation of LAD take-off precluded an antegrade puncturing in the case (when a pre-shape angulated or a reflectable tip microcatheters are not available), changing a strategy to a primary retrograde succeeded in crossing an ambiguous cap from retrograde to the proximal true lumen.

{kind=link}
{kind=link}