Summary
Arteriovenous (AV) fistulae are abnormal connections between arteries and veins bypassing interposed arterioles, capillaries and venules. The occurrence and type of clinical manifestations and treatments for AV fistulae depend on the fistula size and vascular territory involved. Frequently, AV fistulae do not require percutaneous or surgical intervention. When treatment is indicated, provided it is technically feasible, percutaneous intervention is the preferred approach. Methods and equipment depend on the fistula size and location. The following chapter aims to provide an overview of the most commonly encountered fistulae, including clinical manifestations and treatment.
Introduction
An arteriovenous (AV) fistula is an abnormal connection between an artery and a vein bypassing interposed arterioles, capillaries and venules. This typically causes dilatation of the veins it feeds due to transmission of arterial pressure to the venous system. AV fistulae are rare and can be inherited (congenital), or acquired. Acquired fistulae are the consequence of trauma, erosion of an aneurysmal artery into a vein or iatrogenic (e.g., related to arterial and venous puncture for the purpose of catheterisation or to surgical creation of an arteriovenous connection to facilitate haemodialysis). General pathophysiological concepts which apply to any arteriovenous fistula are ischaemia in the territory supplied by the feeding artery and high output failure [11. Shih CH, Liang PC, Chiang FT, Tseng CD, Tseng YZ, Hsu KL. Transcatheter embolization of a huge renal arteriovenous fistula with Amplatzer Vascular Plug. Heart Vessels;25:356-8. ]. The manifestations of ischaemia depend on the location of the fistula (described below for the specific type). The presence, or absence, of signs of systemic hypercirculation (e.g., bounding pulse, low diastolic blood pressure, tachycardia or high output heart failure) depends on the fistula size and magnitude of the shunt. In many clinically relevant fistulae a continuous bruit can be auscultated overlying the fistula. When high output heart failure is diagnosed, auscultation of the abdomen and chest is of utmost importance as a bruit may be the only clue apparent on examination [22. Lekuona I, Laraudogoitia E, Salcedo A, Sadaba M. Congestive heart failure in a hypertensive patient (don’t forget the stethoscope). Lancet. 2001;357:358. ]. In addition to the above, unique, organ-specific symptoms may occur which will be described below.
Coronary fistulae
Coronary fistulae may be either congenital or acquired (e.g., after right heart biopsies in transplant patients or after thoracic surgery). The fistulous connection may occur between any coronary artery or its branches and any of the cardiac chambers or coronary sinus. There may be more than one connection [33. Reidy JF, Anjos RT, Qureshi SA, Baker EJ, Tynan MJ. Transcatheter embolization in the treatment of coronary artery fistulas. J Am Coll Cardiol. 1991;18:187-92. ]. In congenital fistulae, the feeding vessel is most commonly the right coronary (52%) followed by the left anterior descending (LAD) (30%) and the circumflex (LCX) (18%) coronary artery [44. McNamara JJ, Gross RE. Congenital coronary artery fistula. Surgery. 1969;65:59-69. ]. The tract tends to be more tortuous if the fistula originates from the more distal LAD, especially if it enters the left ventricle or if it originates from the proximal RCA and enters into the coronary sinus. When the fistulae arise from a proximal epicardial coronary and enter the right atrium they are generally less tortuous [55. Qureshi SA. Coronary arterial fistulas. Orphanet J Rare Dis. 2006;1:51.
Excellent review of management of coronary artery fistulae.]. The most common entry point is the right ventricle followed by the right atrium, coronary sinus and left ventricle or pulmonary artery [66. Levin DC, Fellows KE, Abrams HL. Hemodynamically significant primary anomalies of the coronary arteries. Angiographic aspects. Circulation. 1978;58:25-34.
Landmark paper on congenital coronary anomalies including fistulae.]. The entry point in fistulae related to previous biopsies is the right ventricle. Many fistulae are asymptomatic and are discovered in childhood due, most frequently, to a continuous murmur and less commonly to a diastolic murmur (in this case the entry chamber is the left ventricle). The murmur is easily mistaken for a patent ductus. However, it is located more caudally compared to a ductus murmur and tends to peak in mid to late diastole. Some fistulae discovered during childhood may close spontaneously. Caution regarding the treatment of asymptomatic fistulae discovered inadvertently in childhood is therefore prudent. When symptoms develop they are commonly related to heart failure from long-standing volume overload (e.g., exertional shortness of breath) [77. Khan MD, Qureshi SA, Rosenthal E, Sharland GK. Neonatal transcatheter occlusion of a large coronary artery fistula with Amplatzer duct occluder. Catheter Cardiovasc Interv. 2003;60:282-6. , 88. Wilde P, Watt I. Congenital coronary artery fistulae: six new cases with a collective review. Clin Radiol. 1980;31:301-11. ] or ischaemia either related to a steal phenomenon [99. Oshiro K, Shimabukuro M, Nakada Y, Chibana T, Yoshida H, Nagamine F, Sunagawa R, Gushiken M, Murakami K, Mimura G. Multiple coronary LV fistulas: demonstration of coronary steal phenomenon by stress thallium scintigraphy and exercise hemodynamics. Am Heart J. 1990;120:217-9. ] or to thrombotic events within the fistula [1010. Ramo OJ, Totterman KJ, Harjula AL. Thrombosed coronary artery fistula as a cause of paroxysmal atrial fibrillation and ventricular arrhythmia. Cardiovasc Surg. 1994;2:720-2. ]. In addition, atrial or ventricular arrhythmias [44. McNamara JJ, Gross RE. Congenital coronary artery fistula. Surgery. 1969;65:59-69. ] and infectious endocarditis [1111. Alkhulaifi AM, Horner SM, Pugsley WB, Swanton RH. Coronary artery fistulas presenting with bacterial endocarditis. Ann Thorac Surg. 1995;60:202-4. ] in association with a coronary fistula have been reported. Though rare, rupture can occur [1212. Bauer HH, Allmendinger PD, Flaherty J, Owlia D, Rossi MA, Chen C. Congenital coronary arteriovenous fistula: spontaneous rupture and cardiac tamponade. Ann Thorac Surg. 1996;62:1521-3. ]. Some fistulae can be visualised echocardiographically and their character identified by cardiac MRI or CT-angiography, but the gold standard diagnostic technique remains coronary angiography. However, precise definition can be difficult due to frequent marked dilatation and/or tortuosity of the feeding coronary and to high flow associated with poor opacification. Under these circumstances the use of catheters with larger diameters or a pigtail catheter positioned in the dilated coronary and power injection may be helpful.
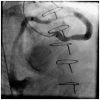
The treatment of asymptomatic fistulae remains controversial. However, many fistulae will increase in size. Therefore, follow-up angiography in conservatively managed patients may by reasonable. Most would probably agree that symptomatic fistulae or those which increase in size or are associated with a significant shunt volume and signs of right or left heart volume overload should be considered for treatment. If this is technically feasible, the first approach should be percutaneous closure. This can be achieved with coils, or vascular plugs depending on the size. It is important to deliver the occluding device as distally into the fistula as possible to avoid ischaemia with more proximal positioning by inadvertent occlusion of the feeding vessel or one of its branches. Coils should be chosen at least 30% larger in diameter than that of the fistula. Figure 1 illustrates coiling of a fistula from the septal perforator to the pulmonary artery.
Coils can be delivered through a guide catheter in the absence of tortuosity and when the tract is short. In longer and tortuous fistulae, deep engagement of bulky guide catheters is associated with a higher risk of coronary or fistula injury. In this latter case, a smaller deliver catheter can be positioned distal into the fistula over a soft-tipped coronary guidewire (0.014 inch) with a hydrophilic shaft. Coils (e.g., 0.018 inch) can then be delivered through the delivery catheter. Alternatively, one may consider delivery of the occlusion device to the distal fistula via the right atrium or ventricle.
This may be the technically favourable approach in the presence of excessive tortuosity. When definition of the anatomy is difficult and it is not clear whether the planned segment to be occluded is distal enough, first a compliant balloon can be inflated in this location to assess whether ischaemia will occur. Frequently, fistulae have high flows and distal embolisation of any of the planned devices is a concern. In such circumstances, distal balloon occlusion during coil delivery is an option to minimise distal embolisation (this approach requires bilateral arterial access and two guide catheters). In technically challenging cases, detachable coils will make the operator’s life much easier as these can be retrieved and repositioned if needed. If and when distal embolisation occurs retrieval with a snare is usually feasible. For large fistulae the use of a vascular plug or pfm coils (pfmmedical, Cologne, Germany) should be considered. Occasionally positioning of the vascular plug or coil in the very distal aspect of the fistula is desirable. To allow positioning, arterial and venous access is frequently helpful for advancement and stable placement of the delivery catheter. In this case, the fistula is wired from the arterial circulation (via the coronary artery) with the final wire position in the fistula outflow (e.g., right ventricle or coronary sinus) and the wire snared via a venous catheter located in the outflow chamber. This will enable advancement of the appropriate catheter to the distal fistula location and a vascular plug or coil can then be delivered. Figure 2 and Figure 3 illustrate this technique. Similar to detachable coils, vascular plugs are retrievable if undersized.
Fistulae related to prior right heart biopsies are usually smaller than congenital fistulae and may be treated with small coils or with a covered stent in the main vessel occluding the feeding side branch. However, the only available covered stent (Jostent®, Abbot Vascular, Santa Clara, CA, USA) is associated with a high rate of restenosis and perhaps thrombosis and, therefore, should not routinely be considered. Though management of coronary fistulae related to right heart biopsies is unclear, most would probably agree that asymptomatic, particularly small fistulae without significant ischaemia are best managed conservatively.
Coronary fistulae
- The most common feeding artery is the right coronary (52%) followed by the left anterior descending (30%) and the circumflex (18%)
- The most common entry site is the right ventricle followed by the right atrium, coronary sinus, left ventricle and pulmonary artery
- Most fistulae are asymptomatic and are diagnosed in childhood due to a murmur. Some discovered in childhood may close spontaneously
- Symptoms are high output failure, ischaemia (related to a steal phenomenon), thrombotic events, ventricular arrhythmias and infectious endocarditis
- Rupture, though it can occur, is rare
- Treatment of asymptomatic fistulae is controversial. Symptomatic fistulae or those that progressively increase in size or are associated with a high shunt volume should be closed
- The treatment of choice is coil or vascular plug embolisation
- Small coronary AV fistulae related to myocardial biopsies should be managed conservatively
Non-coronary cardiac fistulae
Congenital or acquired non-coronary cardiac fistulae are encountered from time to time in cardiological practice. Congenital cardiac fistulae and communications are described in other chapters of this textbook and include patent ductus arteriosus, patent foramen ovale, atrial and ventricular septal defects. Although acquired fistulae are usually iatrogenic, on occasion they can occur as the result of a degenerative or pathological process.
An example of an acquired fistula is a ruptured sinus of Valsalva aneurysm. These rare anomalies are usually caused by a congenital deficiency of muscular and elastic tissue [1313. Abe T, Komatsu S. Surgical repair and long-term results in ruptured sinus of Valsalva aneurysm. Ann Thorac Surg. 1988;46:520-5. ], but can also be acquired as result of conditions affecting the aortic wall such as infections (e.g., syphilis, tuberculosis), or degenerative disease such as atherosclerosis or connective tissue disorders. Rupture usually results in a communication between the right coronary sinus and a right sided heart chamber. Although traditionally these communications have been managed surgically [1313. Abe T, Komatsu S. Surgical repair and long-term results in ruptured sinus of Valsalva aneurysm. Ann Thorac Surg. 1988;46:520-5. ], transcatheter closure has become increasingly used to successfully obliterate the tunnel. Small series have been reported [1414. Arora R, Trehan V, Rangasetty UM, Mukhopadhyay S, Thakur AK, Kalra GS. Transcatheter closure of ruptured sinus of valsalva aneurysm. J Interv Cardiol. 2004;17:53-8. , 1515. Sen S, Chattopadhyay A, Ray M, Bandyopadhyay B. Transcatheter device closure of ruptured sinus of Valsalva: Immediate results and short term follow up. Ann Pediatr Cardiol. 2009;2:79-82.
Series of patients who underwent percutaneous repair of the rare condition of a ruptured sinus of Valsalva.], using AMPLATZER® (AGA Medical Corporation, Plymouth, MN, USA) and other types of occluders.
Other forms of degenerative fistulous communications, associated with a high mortality, are rupture of the ventricular wall causing a ventricular septal defect or a free wall leak into the pericardial cavity. The management of post myocardial infarction ventricular septal defects is described elsewhere.
Free wall ruptures usually occur after myocardial infarction and false aneurysm formation but can also be the result of trauma from a cardiac procedure such as radiofrequency ablation, pacemaker implantation or a cardiac biopsy procedure. Although these complications often result in tamponade treated by pericardiocentesis, surgical repair of a ventricular rupture is often required and has a significant associated mortality [1616. Frances C, Romero A, Grady D. Left ventricular pseudoaneurysm. J Am Coll Cardiol. 1998;32:557-61. ].
An alternative strategy is to consider percutaneous closure. A number of successful cases have been reported [1717. Gladding PA, Ruygrok PN, Greaves SC, Gerber IL, Hamer AW. Images in cardiovascular medicine. Percutaneous closure of a left ventricular free-wall rupture site. Circulation. 2006;113:e748-9. , 1818. Harrison W, Ruygrok PN, Greaves S, Wijesinghe N, Charleson H, Wade C, Devlin G. Percutaneous closure of left ventricular free wall rupture with associated false aneurysm to prevent cardioembolic stroke. Heart Lung Circ. 2008;17:250-3. ]. In most, an AMPLATZER Atrial Septal Defect (ASD) or post infarction Ventricular Septal Defect (VSD) occluder was used to successfully occlude the neck of the false aneurysm although other similar devices could be considered ( Figure 4 ).
Cardiac fistulous communications are either due to trauma (e.g., gunshot wound or stabbing) or iatrogenic related to cardiac surgery, percutaneous coronary intervention, pacemaker implantation, electrophysiological and structural heart disease procedures or endomyocardial biopsy. The frequency of these complications may be increasing with the growing use of percutaneous methods to treat structural heart disease and the transseptal puncture technique to access the left heart for procedures such as left atrial appendage occlusion, mitral valve repair and pulmonary vein isolation. Usually the smaller catheter, dilator or wire tip perforations seal and cease bleeding spontaneously, facilitated by the administration of protamine if unfractionated heparin was given.
A small number of cases describing the percutaneous closure of ventricular septal defects, resulting from a knife stab, using an AMPLATZER® occluder have been reported [1919. Berry C, Hillis WS, Knight WB. Transcatheter closure of a ventricular septal defect resulting from knife stabbing using the Amplatzer muscular VSD occluder. Catheter Cardiovasc Interv. 2006;68:153-6. ]. This suggests that percutaneous closure of other iatrogenic fistulous connections caused in this way, such as a free ventricular wall rupture, could also conceivably be treated percutaneously.
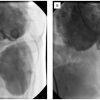
Transseptal puncture, particularly in hearts with dilated or distorted chambers, can be challenging and, on occasion, complicated by a wire and or dilator terminating in a chamber or space other than the left atrium. An illustrative case is shown in Figure 5 where, during a transseptal puncture, the wire and dilator passed through the pericardial reflection into the ascending aorta resulting in tamponade and haemodynamic compromise. The torrential bleeding was arrested by deploying a 4 mm AMPLATZER® (ASD) occluder across the communication with no sequelae and an excellent clinical outcome.
Finally, another form of iatrogenic fistulous connection encountered from time to time is a bypass graft inadvertently anastomosed onto a coronary vein. An example of this situation is shown in Figure 6 with contrast injected into a saphenous bypass graft draining into the right atrium via the coronary sinus. If significant shunting occurs or there is concern about increasing dilatation of the bypass graft, it can be occluded percutaneously, as has been described for coronary fistulae in an earlier section of this chapter [2020. Lopez JJ, Kuntz RE, Baim DS, Johnson RG, Kim D. Percutaneous occlusion of an iatrogenic aortosaphenous vein – coronary vein fistula via retrograde coronary sinus approach. Cathet Cardiovasc Diagn. 1996;37:339-41. ].
Non-coronary cardiac fistulae in general, and in particular those caused by circular objects such as a wire, dilator, catheter or sheath, tend to be straight rather than tortuous, and therefore consideration may be given to closure employing percutaneous catheter based techniques. This is of course dependent on the rapid accessibility of equipment and expertise, the acuity of the patient and the relative risk of a surgical approach.
Non-coronary cardiac fistulae
- These include fistulae related to rupture of a sinus of Valsalva aneurysm (usually of the right coronary sinus) into a right heart chamber
- Traditionally surgery has been the treatment of choice
- Percutaneous repair has been demonstrated (e.g., with an AMPLATZER® occlude)
- Similarly closure of ventricular pseudoaneurysms with ASD or VSD occluders has been described
Pulmonary arteriovenous malformations
The most common type of pulmonary arteriovenous fistulae are congenital pulmonary AV malformations, typically (80%) as part of hereditary haemorrhagic telangiectasia (HHT), an autosomal dominant disorder associated with AV-fistulae [2121. Guttmacher AE, Marchuk DA, White RI Jr. Hereditary hemorrhagic telangiectasia. N Engl J Med. 1995;333: 918-24. , 2222. Faughnan ME, Granton JT, Young LH. The pulmonary vascular complications of hereditary haemorrhagic telangiectasia. Eur Respir J. 2009;33:1186-94.
Excellent review of the vascular complications of the most common disorder (hereditary telangiectasia) causing pulmonary arteriovenous fistulae.]. The risk of developing a pulmonary AV fistula in patients with HHT is 20% to 40% and is higher in individuals with endoglin mutation [2323. Mager JJ, Overtoom TT, Blauw H, Lammers JW, Westermann CJ. Embolotherapy of pulmonary arteriovenous malformations: long-term results in 112 patients. J Vasc Interv Radiol. 2004;15:451-6.
Long-term results in a large series of patients with pulmonary arteriovenous fistulae who underwent percutaneous embolisation., 2424. Lesca G, Olivieri C, Burnichon N, Pagella F, Carette MF, Gilbert-Dussardier B, Goizet C, Roume J, Rabilloud M, Saurin JC, Cottin V, Honnorat J, Coulet F, Giraud S, Calender A, Danesino C, Buscarini E, Plauchu H; French-Italian-Rendu-Osler Network. Genotype-phenotype correlations in hereditary hemorrhagic telangiectasia: data from the French-Italian HHT network. Genet Med. 2007;9:14-22. ]. The risk of paradoxical embolism related to venous thrombi or to thrombi originating at the malformation is significant and the potential consequences are grave including peripheral or cerebral embolism causing a stroke and/or cerebral abscess [2323. Mager JJ, Overtoom TT, Blauw H, Lammers JW, Westermann CJ. Embolotherapy of pulmonary arteriovenous malformations: long-term results in 112 patients. J Vasc Interv Radiol. 2004;15:451-6.
Long-term results in a large series of patients with pulmonary arteriovenous fistulae who underwent percutaneous embolisation., 2525. Cottin V, Chinet T, Lavole A, Corre R, Marchand E, Reynaud-Gaubert M, Plauchu H, Cordier JF; Groupe d’Etudes et de Recherche sur les Maladies “Orphelines” Pulmonaires (GERM“O”P). Pulmonary arteriovenous malformations in hereditary hemorrhagic telangiectasia: a series of 126 patients. Medicine (Baltimore). 2007;86:1-17. , 2626. White RI Jr, Lynch-Nyhan A, Terry P, Buescher PC, Farmlett EJ, Charnas L, Shuman K, Kim W, Kinnison M, Mitchell SE. Pulmonary arteriovenous malformations: techniques and long-term outcome of embolotherapy. Radiology. 1988;169:663-9. , 2727. Moussouttas M, Fayad P, Rosenblatt M, Hashimoto M, Pollak J, Henderson K, Ma TY, White RI. Pulmonary arteriovenous malformations: cerebral ischemia and neurologic manifestations. Neurology. 2000;55:959-64. , 2828. White RI Jr, Pollak JS, Wirth JA. Pulmonary arteriovenous malformations: diagnosis and transcatheter embolotherapy. J Vasc Interv Radiol. 1996;7:787-804. ]. Further, haemoptysis and hypoxemia as well as high output failure have been reported depending on the shunt size [2323. Mager JJ, Overtoom TT, Blauw H, Lammers JW, Westermann CJ. Embolotherapy of pulmonary arteriovenous malformations: long-term results in 112 patients. J Vasc Interv Radiol. 2004;15:451-6.
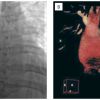
Long-term results in a large series of patients with pulmonary arteriovenous fistulae who underwent percutaneous embolisation., 2525. Cottin V, Chinet T, Lavole A, Corre R, Marchand E, Reynaud-Gaubert M, Plauchu H, Cordier JF; Groupe d’Etudes et de Recherche sur les Maladies “Orphelines” Pulmonaires (GERM“O”P). Pulmonary arteriovenous malformations in hereditary hemorrhagic telangiectasia: a series of 126 patients. Medicine (Baltimore). 2007;86:1-17. , 2626. White RI Jr, Lynch-Nyhan A, Terry P, Buescher PC, Farmlett EJ, Charnas L, Shuman K, Kim W, Kinnison M, Mitchell SE. Pulmonary arteriovenous malformations: techniques and long-term outcome of embolotherapy. Radiology. 1988;169:663-9. , 2727. Moussouttas M, Fayad P, Rosenblatt M, Hashimoto M, Pollak J, Henderson K, Ma TY, White RI. Pulmonary arteriovenous malformations: cerebral ischemia and neurologic manifestations. Neurology. 2000;55:959-64. ]. The malformations are categorised as simple or complex depending on whether they are fed by a single or multiple pulmonary arteries. Further, malformations can be single, limited to one lobe or segment or multiple involving more than one lobe or segment. Figure 7 illustrates a complex (fed by more than one pulmonary artery) single (limited to the lower lobe) AV fistula. Commonly, more than one AV fistula is present with an average of three [2929. Pollak JS, Saluja S, Thabet A, Henderson KJ, Denbow N, White RI Jr. Clinical and anatomic outcomes after embolotherapy of pulmonary arteriovenous malformations. J Vasc Interv Radiol. 2006;17:35-44;quiz 45. ]. Though a pulmonary AV fistula can be diagnosed by the presence of a pulmonary bruit, this can be detected in only a minority of HHT patients with AV fistulae. The best screening test is contrast echocardiography which has a sensitivity of >90% [3030. Cottin V, Plauchu H, Bayle JY, Barthelet M, Revel D, Cordier JF. Pulmonary arteriovenous malformations in patients with hereditary hemorrhagic telangiectasia. Am J Respir Crit Care Med. 2004;169:994-1000. , 3131. Nanthakumar K, Graham AT, Robinson TI, Grande P, Pugash RA, Clarke JA, Hutchison SJ, Mandzia JL, Hyland RH, Faughnan ME. Contrast echocardiography for detection of pulmonary arteriovenous malformations. Am Heart J. 2001;141:243-6. ]. This can be complemented by computed tomography [3232. Curie A, Lesca G, Cottin V, Edery P, Bellon G, Faughnan ME, Plauchu H. Long-term follow-up in 12 children with pulmonary arteriovenous malformations: confirmation of hereditary hemorrhagic telangiectasia in all cases. J Pediatr. 2007;151:299-306. ].
Surgical therapy is associated with significant morbidity and mortality and therefore, when technically feasible, percutaneous embolisation is the preferred treatment modality. Most would recommend the treatment of AV fistulae supplied by a feeding artery >3 mm to prevent embolic events [3333. Faughnan ME, Palda VA, Garcia-Tsao G, Geisthoff UW, McDonald J, Proctor DD, Spears J, Brown DH, Buscarini E, Chesnutt MS, Cottin V, Ganguly A, Gossage JR, Guttmacher AE, Hyland RH, Kennedy SJ, Korzenik J, Mager JJ, Ozanne AP, Piccirillo JF, Picus D, Plauchu H, Porteous ME, Pyeritz RE, Ross DA, Sabba C, Swanson K, Terry P, Wallace MC, Westermann CJ, White RI, Young LH, Zarrabeitia R. International guidelines for the diagnosis and management of hereditary hemorrhagic telangiectasia. J Med Genet. 2011;48:73-87.
Guidelines for the management of pulmonary arteriovenous fistulae.]. The most common approaches are coil embolisation, implantation of a vascular plug, sponge embolisation or a combination of the above. After systemic anticoagulation (e.g., with intravenous heparin), subselective catheterisation of the feeding segmental pulmonary artery can be performed via femoral (or less commonly internal jugular) venous access followed by placement of a long 6 Fr to 8 Fr sheath into the main pulmonary artery. This will facilitate exchange or delivery of equipment and minimises ventricular ectopy. Over a wire, a guide catheter (e.g., multipurpose or hockey stick catheter) can be positioned into the segmental pulmonary artery and coils or a vascular plug delivered via the catheter. Alternatively, for the placement of coils, a delivery catheter can be advanced through the guide catheter and coils delivered via the delivery catheter. If coils are used, typically, the diameter of the unconstrained coils should be two millimetres larger than the feeding vessel. If a smaller diameter is chosen, the risk of embolisation increases, if too large a diameter is chosen, the coils may not fully unfold and incomplete embolisation may be the consequence. When multiple AV malformations are present, it is common practice to treat them in a staged fashion to minimise the risk of pulmonary infection as a consequence of pulmonary infarction. The interval is typically 4 to 6 weeks. Contraindications to pulmonary embolisation are an active, particularly pulmonary, infection and greater than moderate pulmonary hypertension. In the presence of normal pulmonary artery pressure significant elevation of the pulmonary artery pressure after embolotherapy is very unlikely [3434. Shovlin CL, Tighe HC, Davies RJ, Gibbs JS, Jackson JE. Embolisation of pulmonary arteriovenous malformations: no consistent effect on pulmonary artery pressure. Eur Respir J. 2008;32:162-9. ]. If pulmonary hypertension is present prior to embolisation and the feeding artery and pulmonary segment are large, the consequences of embolisation on the pulmonary artery pressure should first be assessed with balloon occlusion and measurement of pulmonary artery pressure and abandoned if the mean pulmonary artery pressure increases by more than 5 mmHg. A small subset of HHT patients have pulmonary hypertension with a vasculopathy similar to that which can be seen in primary pulmonary hypertension [3535. Abdalla SA, Letarte M. Hereditary haemorrhagic telangiectasia: current views on genetics and mechanisms of disease. J Med Genet. 2006;43:97-110. , 3636. Abdalla SA, Gallione CJ, Barst RJ, Horn EM, Knowles JA, Marchuk DA, Letarte M, Morse JH. Primary pulmonary hypertension in families with hereditary haemorrhagic telangiectasia. Eur Respir J. 2004;23:373-7. ] and this should be excluded prior to embolisation. The reported technical success rate of embolisation is very high and the recurrence risk low. The incidence of complications is generally lower with endovascular therapy than surgery. Pleurisy (pleuritic chest pain and low grade fever) and pleural effusion are not uncommon 3 to 6 days after the procedure (10% to 35%) but usually self-limiting [2626. White RI Jr, Lynch-Nyhan A, Terry P, Buescher PC, Farmlett EJ, Charnas L, Shuman K, Kim W, Kinnison M, Mitchell SE. Pulmonary arteriovenous malformations: techniques and long-term outcome of embolotherapy. Radiology. 1988;169:663-9. , 3131. Nanthakumar K, Graham AT, Robinson TI, Grande P, Pugash RA, Clarke JA, Hutchison SJ, Mandzia JL, Hyland RH, Faughnan ME. Contrast echocardiography for detection of pulmonary arteriovenous malformations. Am Heart J. 2001;141:243-6. , 3737. Lee DW, White RI Jr, Egglin TK, Pollak JS, Fayad PB, Wirth JA, Rosenblatt MM, Dickey KW, Burdge CM. Embolotherapy of large pulmonary arteriovenous malformations: long-term results. Ann Thorac Surg. 1997; 64:930-9; discussion 939-40. ], however, death as a result of infection related to pulmonary infarction after embolisation of a large pulmonary segment has been reported. Other complications related to vascular access and distal (systemic) embolisation are uncommon [2323. Mager JJ, Overtoom TT, Blauw H, Lammers JW, Westermann CJ. Embolotherapy of pulmonary arteriovenous malformations: long-term results in 112 patients. J Vasc Interv Radiol. 2004;15:451-6.
Long-term results in a large series of patients with pulmonary arteriovenous fistulae who underwent percutaneous embolisation., 2626. White RI Jr, Lynch-Nyhan A, Terry P, Buescher PC, Farmlett EJ, Charnas L, Shuman K, Kim W, Kinnison M, Mitchell SE. Pulmonary arteriovenous malformations: techniques and long-term outcome of embolotherapy. Radiology. 1988;169:663-9. , 2828. White RI Jr, Pollak JS, Wirth JA. Pulmonary arteriovenous malformations: diagnosis and transcatheter embolotherapy. J Vasc Interv Radiol. 1996;7:787-804. , 3737. Lee DW, White RI Jr, Egglin TK, Pollak JS, Fayad PB, Wirth JA, Rosenblatt MM, Dickey KW, Burdge CM. Embolotherapy of large pulmonary arteriovenous malformations: long-term results. Ann Thorac Surg. 1997; 64:930-9; discussion 939-40. ]. When embolisation of coils occurs it is usually related to undersizing or to a high flow velocity through the fistula. To prevent embolisation from a high flow rate, consideration should be given to proximal balloon occlusion during coil delivery. Embolised coils most commonly lodge in the internal carotid, coeliac, superior mesenteric or iliac circulation but in most instances can be snared without difficulty. After successful occlusion of AV fistulae, recanalisation can occur (up to 17% in one study [2929. Pollak JS, Saluja S, Thabet A, Henderson KJ, Denbow N, White RI Jr. Clinical and anatomic outcomes after embolotherapy of pulmonary arteriovenous malformations. J Vasc Interv Radiol. 2006;17:35-44;quiz 45. ]) and, therefore, follow-up is recommended with contrast echo and or computed tomography [2323. Mager JJ, Overtoom TT, Blauw H, Lammers JW, Westermann CJ. Embolotherapy of pulmonary arteriovenous malformations: long-term results in 112 patients. J Vasc Interv Radiol. 2004;15:451-6.
Long-term results in a large series of patients with pulmonary arteriovenous fistulae who underwent percutaneous embolisation., 2929. Pollak JS, Saluja S, Thabet A, Henderson KJ, Denbow N, White RI Jr. Clinical and anatomic outcomes after embolotherapy of pulmonary arteriovenous malformations. J Vasc Interv Radiol. 2006;17:35-44;quiz 45. , 3838. Lee WL, Graham AF, Pugash RA, Hutchison SJ, Grande P, Hyland RH, Faughnan ME. Contrast echocardiography remains positive after treatment of pulmonary arteriovenous malformations. Chest. 2003;123:351-8. ] (e.g., one year after treatment and less frequently thereafter). Given the risk of recanalisation and cerebral abscess formation regardless of the size of untreated residual fistulae, antibiotic prophylaxis should be recommended to patients with AV-malformations despite successful embolotherapy [3939. Gossage JR, Kanj G. Pulmonary arteriovenous malformations. A state of the art review. Am J Respir Crit Care Med. 1998;158:643-61. ]. Further, air filters are recommended with any intravenous infusions to prevent air embolism and cerebral ischaemic events and scuba diving should be discouraged [3838. Lee WL, Graham AF, Pugash RA, Hutchison SJ, Grande P, Hyland RH, Faughnan ME. Contrast echocardiography remains positive after treatment of pulmonary arteriovenous malformations. Chest. 2003;123:351-8. ]. Figure 7 illustrates two pulmonary AV fistulae in the left lower lobe, the smaller of which is occluded with a 4 mm AMPLATZER® Vascular Plugs (AGA Medical Corporation) and the larger with an 8 mm AMPLATZER® Vascular Plug delivered via a multipurpose catheter positioned in the respective segmental pulmonary arteries.
Though data comparing percutaneous embolisation of pulmonary AV malformations to no therapy in a controlled randomised fashion does not exist, there is ample evidence based on case series and reports that this therapy reduces the likelihood of cerebral embolisation, abscess formation, haemoptysis or high output failure [2626. White RI Jr, Lynch-Nyhan A, Terry P, Buescher PC, Farmlett EJ, Charnas L, Shuman K, Kim W, Kinnison M, Mitchell SE. Pulmonary arteriovenous malformations: techniques and long-term outcome of embolotherapy. Radiology. 1988;169:663-9. , 3131. Nanthakumar K, Graham AT, Robinson TI, Grande P, Pugash RA, Clarke JA, Hutchison SJ, Mandzia JL, Hyland RH, Faughnan ME. Contrast echocardiography for detection of pulmonary arteriovenous malformations. Am Heart J. 2001;141:243-6. , 3737. Lee DW, White RI Jr, Egglin TK, Pollak JS, Fayad PB, Wirth JA, Rosenblatt MM, Dickey KW, Burdge CM. Embolotherapy of large pulmonary arteriovenous malformations: long-term results. Ann Thorac Surg. 1997; 64:930-9; discussion 939-40. ]. Given the high incidence of potentially life-threatening events in the absence of treatment and the relatively low risk and high rate of technical success with endovascular therapy, comparison to placebo would be unethical and will therefore never be performed.
Pulmonary AV fistulae
- Pulmonary AV fistulae are a typically a manifestation of (autosomal dominant) hereditary haemorrhagic telangiectasia (HHT)
- The risk of AV malformations in patients with HHT is higher in the presence of the endoglin mutation
- Symptoms and signs include haemoptysis, paradoxical embolism, right heart failure or hypoxemia. A bruit by auscultation is heard only in the minority of patients
- More commonly than not fistulae are multiple (average: three)
- Contrast echocardiography is an excellent screening test (sensitivity >90%)
- Fistula closure is recommended even for asymptomatic fistulae fed by an artery of >3 mm diameter to prevent embolic events. Most would recommend staged closure when more than one fistula is present
- Contraindications to fistula closure are: active pulmonary infection and greater than moderate pulmonary hypertension
- The treatment modality of choice is coil or vascular plug embolisation
- Potential complications unique to this procedure are: pleuritic chest pain or pleural effusion (10% to 35%) and pulmonary infarction with subsequent infection
- Recurrence (up to 17%) is not uncommon. Follow-up contrast echo or chest CT is therefore recommended
Renal arteriovenous fistulae
Arteriovenous fistulae in this location are rare. They may be acquired, congenital or idiopathic. Congenital fistulae are most commonly located in the renal medulla and frequently consist of a network of small tortuous arteries with multiple venous communications. Arteriovenous fistulae are most commonly acquired (70%) [4040. Crotty KL, Orihuela E, Warren MM. Recent advances in the diagnosis and treatment of renal arteriovenous malformations and fistulas. J Urol. 1993;150:1355-9. ] and can be related to trauma [4141. Darcq C, Guy L, Garcier JM, Boyer L, Boiteux JP. [Post-traumatic secondary arteriovenous fistulae of the kidney and their embolization. Report of 3 cases]. Prog Urol. 2002;12:21-6. ], erosion of an arterial aneurysm (e.g., fibromuscular dysplasia [4242. Altit R, Brown DB, Gardiner GA. Renal artery aneurysm and arteriovenous fistula associated with fibromuscular dysplasia: successful treatment with detachable coils. J Vasc Interv Radiol. 2009;20:1083-6. ] or atherosclerotic) into a renal vein, procedures (e.g., fine needle biopsy [4343. Sasaki N, Joashi UC, Vergara M, Saland JM, Love BA. Postrenal biopsy AVM leading to severe hypertension and dilated cardiomyopathy. Pediatr Nephrol. 2009;24:2459-62. ] or percutaneous nephrostomy) or previous surgery. Fistulae are readily diagnosed with renal ultrasonography. The most common symptoms are haematuria [4141. Darcq C, Guy L, Garcier JM, Boyer L, Boiteux JP. [Post-traumatic secondary arteriovenous fistulae of the kidney and their embolization. Report of 3 cases]. Prog Urol. 2002;12:21-6. ], hypertension [4343. Sasaki N, Joashi UC, Vergara M, Saland JM, Love BA. Postrenal biopsy AVM leading to severe hypertension and dilated cardiomyopathy. Pediatr Nephrol. 2009;24:2459-62. , 4444. Paschalis-Purtak K, Januszewicz M, Rokicki A, Puciłowska B, Imiela J, Cybulska I, Cies’la W, Prejbisz A, Szostek M, Januszewicz A. Arteriovenous fistula of the kidney: a case report of 47-year-old female patient treated by embolisation. J Hum Hypertens. 2003;17:293-6. , 4545. Arguelles Garcia B, Medrano S, Meilan Martinez A, Vega F. [Renal arteriovenous fistulas as a cause of refractory hypertension]. Radiologia. 2009;51:500-3. ] and high output heart failure [11. Shih CH, Liang PC, Chiang FT, Tseng CD, Tseng YZ, Hsu KL. Transcatheter embolization of a huge renal arteriovenous fistula with Amplatzer Vascular Plug. Heart Vessels;25:356-8. , 4343. Sasaki N, Joashi UC, Vergara M, Saland JM, Love BA. Postrenal biopsy AVM leading to severe hypertension and dilated cardiomyopathy. Pediatr Nephrol. 2009;24:2459-62. ]. Hypertension occurs in up to 40% of patients with fistulae and refractory hypertension, related to a renal arteriovenous fistulae has been reported [4646. Ullian ME, Molitoris BA. Bilateral congenital renal arteriovenous fistulas. Clin Nephrol. 1987;27:293-7. ]. In theory, hypertension may be related to a steal phenomenon with subsequent hypoperfusion and renin hypersecretion of the renal segment supplied by the renal artery feeding the fistula. However, available studies demonstrate normal renal vein renin levels without lateralisation [4646. Ullian ME, Molitoris BA. Bilateral congenital renal arteriovenous fistulas. Clin Nephrol. 1987;27:293-7. , 4747. Abud O, Chechile G, Sole-Balcells F. Aneurysm and arteriovenous malformation. In: Novick A, Scoble J, Hamilton G, eds. Renal Vascular Disease. London: WB Saunders, 1996:35-46. ]. Little data is available on the likelihood of cure or hypertension improvement after surgical or endovascular therapy. The blood pressure response appears to be variable with some reports suggesting a higher likelihood of improvement in patients with acquired traumatic fistulae than with congenital fistulae [4848. Morin RP, Dunn EJ, Wright CB. Renal arteriovenous fistulas: a review of etiology, diagnosis, and management. Surgery. 1986;99:114-8. , 4949. Corr P, Hacking G. Embolization in traumatic intrarenal vascular injuries. Clin Radiol. 1991;43:262-4. , 5050. Phadke RV, Sawlani V, Rastogi H, Kumar S, Roy S, Baijal SS, Babu VR, Ahlawat R, Kher V, Gujral RB. Iatrogenic renal vascular injuries and their radiological management. Clin Radiol. 1997;52:119-23. ]. The physical examination almost invariably reveals an abdominal bruit [4040. Crotty KL, Orihuela E, Warren MM. Recent advances in the diagnosis and treatment of renal arteriovenous malformations and fistulas. J Urol. 1993;150:1355-9. ]. Asymptomatic fistulae can be managed conservatively. Importantly, acquired fistulae related to surgery, penetrating trauma or renal biopsy can resolve spontaneously [5151. Tarkington MA, Matsumoto AH, Dejter SW, Regan JB. Spectrum of renal vascular malformation. Urology. 1991;38:297-300. ].
The treatment modality depends on the size and location of the fistula. Large fistulae can be occluded with a vascular plug with or without coils [11. Shih CH, Liang PC, Chiang FT, Tseng CD, Tseng YZ, Hsu KL. Transcatheter embolization of a huge renal arteriovenous fistula with Amplatzer Vascular Plug. Heart Vessels;25:356-8. , 4343. Sasaki N, Joashi UC, Vergara M, Saland JM, Love BA. Postrenal biopsy AVM leading to severe hypertension and dilated cardiomyopathy. Pediatr Nephrol. 2009;24:2459-62. , 5252. Campbell JE, Davis C, Defade BP, Tierney JP, Stone PA. Use of an amplatzer vascular plug for transcatheter embolization of a renal arteriovenous fistula. Vascular. 2009;17:40-3. ]. In this case, an 8 Fr sheath and guide catheter can be used for cannulation. If the feeding vessel is of large size, a 0.035 inch guide wire can be advanced into the fistula and exchanged over a 4 Fr catheter for a stiffer wire if necessary. This wire will allow positioning of a 6 Fr guide catheter into the feeding vessel and deployment of the vascular plug. If device migration is of concern, isolation of the vascular segment to be treated may be accomplished with balloon inflation in the feeding and draining vessel [11. Shih CH, Liang PC, Chiang FT, Tseng CD, Tseng YZ, Hsu KL. Transcatheter embolization of a huge renal arteriovenous fistula with Amplatzer Vascular Plug. Heart Vessels;25:356-8. ]. Smaller fistula tracts can be occluded with vascular coils [4141. Darcq C, Guy L, Garcier JM, Boyer L, Boiteux JP. [Post-traumatic secondary arteriovenous fistulae of the kidney and their embolization. Report of 3 cases]. Prog Urol. 2002;12:21-6. , 5353. Banerji JS, Aswathaman K, Mani SE. Delayed presentation of traumatic renal AV fistula managed by coil embolization. Saudi J Kidney Dis Transpl. ;21:531-2. ]. If the target vessel is of larger calibre and the flow is significant, distal embolisation is a concern. In this case, consideration can be given to controlled release detachable coils. Other techniques include the deployment of a vascular plug first followed by coil delivery with the vascular plug acting as a cage. Alternatively, if the anatomy allows (e.g., rather perpendicular take-off of the feeding artery from the parent artery), a stent can be placed in the parent artery first and coils can then be delivered through the stent into the feeding artery.
Renal arteriovenous fistulae
- Renal AV fistulae are rare. Most are acquired (70%) (iatrogenic or trauma)
- Symptoms and signs include haematuria, hypertension (in 40% of patients) and high output failure. An abdominal bruit is common
- Acquired fistulae frequently resolve spontaneously. Most asymptomatic fistulae do not need to be treated
- The treatment method of choice is percutaneous coil or vascular plug delivery depending on the fistula size
Hepatic arteriovenous fistulae
Fistulae can occur between any intestinal or hepatic arteries and the portal or hepatic veins. The most common inflow vessel is the hepatic artery (60%) followed by the splenic artery (11%) and superior mesenteric artery (10%) [5454. Vauthey JN, Tomczak RJ, Helmberger T, Gertsch P, Forsmark C, Caridi J, Reed A, Langham MR Jr, Lauwers GY, Goffette P, Lerut J. The arterioportal fistula syndrome: clinicopathologic features, diagnosis, and therapy. Gastroenterology. 1997;113: 1390-401.
Excellent review on clinical features and treatment of arterioportal fistulae.]. Fistulae connecting the hepatic artery to the portal vein can be congenital or the result of prior trauma, procedures (e.g., biopsies) or surgery. When symptomatic, portal hypertension (leading to oesophageal varices, ascites and splenomegaly) [5555. Foley WJ, Turcotte JG, Hoskins PA, Brant RL, Ause RG. Intrahepatic Arteriovenous Fistulas between the Hepatic Artery and Portal Vein. Ann Surg. 1971;174:849-55. , 5656. Roux P, Hebert T, Anghelescu D, Kerneis J, Nonent M. Endovascular treatment of arterioportal fistula with the amplatzer occlusion device. J Vasc Interv Radiol. 2009;20:685-7. ], intestinal or pancreatic ischaemia (from a steal phenomenon) with abdominal pain and/or diarrhoea [5757. Chen Q, Tack C, Morcos M, Ruggiero M, Schlossberg P, Fogel J, Weng LJ, Farkas J. Embolotherapy of an arterioportal fistula. Cardiovasc Intervent Radiol. 2007;30:1047-51. ] and haemobilia or gastrointestinal bleeding are the most frequent symptoms. Due to a rather high hepatic sinusoidal resistance, heart failure is uncommon. However, right heart failure and pulmonary hypertension [5858. Chua DY, Pavillion G, Tay KH, Tan JL, Chung AY. Pulmonary hypertension: an unusual presentation of an iatrogenic hepatic arterioportal fistula and its successful resolution post-embolotherapy. Am Surg. 2009;75:511-4. ] have been reported and may be more likely in younger patients due to a lower hepatosinusoidal resistance [5959. Levick CB, Rubie J. Haemangioendothelioma of the liver simulating congenital heart disease in an infant. Arch Dis Child. 1953;28:49-51. ]. If the fistulae are related to trauma, the symptoms generally occur within two years but some do not become clinically apparent for a decade or even longer after the causative event [6060. Missavage AE, Jones AM, Walt AJ, Hans B, Jacobs LA. Traumatic hepatic arteriovenous fistula causing portal hypertension and variceal bleeding. J Trauma. 1984;24:355-8. ]. Fistulae which are located in the periphery can resolve spontaneously whereas more centrally located fistulae normally do not. Fistulae can be diagnosed with ultrasound which typically shows a dilated or aneurysmatic portal vein and arterialisation of the flow pattern in the portal vein as well as in some cases hepatofugal flow (flow directed away from the liver) or with contrast CT or MRI demonstrating premature opacification of the portal vein in the arterial phase. Contrast CT imaging is more sensitive than ultrasound imaging for the detection of smaller fistulae [6161. Bolognesi M, Sacerdoti D, Bombonato G, Chiesura-Corona M, Merkel C, Gatta A. Arterioportal fistulas in patients with liver cirrhosis: usefulness of color Doppler US for screening. Radiology. 2000;216:738-43. ]. Angiography remains the gold standard which demonstrates early filling of the portal vein on aortic or coeliac trunk injection.
The best treatment strategy is controversial. However, it is reasonable to manage small, especially peripheral, fistulae conservatively with ultrasound follow-up as many will close spontaneously [6262. Lumsden AB, Allen RC, Sreeram S, Atta H, Salam A. Hepatic arterioportal fistula. Am Surg. 1993;59:722-6. , 6363. Jabbour N, Reyes J, Zajko A, Nour B, Tzakis AG, Starzl TE, Van Thiel DH. Arterioportal fistula following liver biopsy. Three cases occurring in liver transplant recipients. Dig Dis Sci. 1995;40:1041-4. ]. Most would probably agree that symptomatic fistulae, asymptomatic fistulae associated with portal hypertension or fistulae which increase in size should be treated [5454. Vauthey JN, Tomczak RJ, Helmberger T, Gertsch P, Forsmark C, Caridi J, Reed A, Langham MR Jr, Lauwers GY, Goffette P, Lerut J. The arterioportal fistula syndrome: clinicopathologic features, diagnosis, and therapy. Gastroenterology. 1997;113: 1390-401.
Excellent review on clinical features and treatment of arterioportal fistulae., 6363. Jabbour N, Reyes J, Zajko A, Nour B, Tzakis AG, Starzl TE, Van Thiel DH. Arterioportal fistula following liver biopsy. Three cases occurring in liver transplant recipients. Dig Dis Sci. 1995;40:1041-4. ]. In addition, extrahepatic arterioportal fistulae do not usually close spontaneously and therefore should be treated regardless of the presence or absence of symptoms [6262. Lumsden AB, Allen RC, Sreeram S, Atta H, Salam A. Hepatic arterioportal fistula. Am Surg. 1993;59:722-6. , 6464. Strodel WE, Eckhauser FE, Lemmer JH, Whitehouse WM Jr, Williams DM. Presentation and perioperative management of arterioportal fistulas. Arch Surg. 1987;122:563-71. ]. The rational for treatment in asymptomatic fistulae is the prevention of hepatoportal sclerosis, portal hypertension and perhaps, liver cirrhosis [5454. Vauthey JN, Tomczak RJ, Helmberger T, Gertsch P, Forsmark C, Caridi J, Reed A, Langham MR Jr, Lauwers GY, Goffette P, Lerut J. The arterioportal fistula syndrome: clinicopathologic features, diagnosis, and therapy. Gastroenterology. 1997;113: 1390-401.
Excellent review on clinical features and treatment of arterioportal fistulae., 6464. Strodel WE, Eckhauser FE, Lemmer JH, Whitehouse WM Jr, Williams DM. Presentation and perioperative management of arterioportal fistulas. Arch Surg. 1987;122:563-71. ]. Most frequently, the fistulae can be treated with coil embolisation with or without adjunctive agents. Selective hepatic artery cannulation can usually be carried out with the help of a Cobra (Cook Medical, Bloomington, IN, USA) or Simmons catheter (Cook Medical) and hydrophilic guidewire and the coils delivered via a microcatheter. Alternatively, particularly in larger fistulae with high flow, a vascular plug can be deployed [5656. Roux P, Hebert T, Anghelescu D, Kerneis J, Nonent M. Endovascular treatment of arterioportal fistula with the amplatzer occlusion device. J Vasc Interv Radiol. 2009;20:685-7. ]. Potential complications related to the procedure include liver failure (from liver infarction), portal vein thrombosis, biliary fistula or stricture formation and stroke [5656. Roux P, Hebert T, Anghelescu D, Kerneis J, Nonent M. Endovascular treatment of arterioportal fistula with the amplatzer occlusion device. J Vasc Interv Radiol. 2009;20:685-7. ]. However, the consequences of accidental hepatic artery embolisation are usually benign even if flow in the hepatic artery is completely interrupted as most of the hepatic circulation and half of the oxygen supply is usually provided by the portal vein. The exception is previous compromise in hepatic function with abnormal reserve under which circumstances liver failure related to an infarct can occur. Likewise, when the vessel feeding the fistula is the splenic artery, embolisation (or surgical ligation) is usually safe due to collateral blood flow from the left gastroepiploic or short epigastric arteries.
At this point, hereditary haemorrhagic telangiectasia (HHT), previously discussed under pulmonary arteriovenous fistulae, merits some discussion. When sensitive imaging techniques are used (e.g., computed tomography) arteriovenous fistulae in the liver can be seen in up to 75% of patients [6565. Buonamico P, Suppressa P, Lenato GM, Pasculli G, D’Ovidio F, Memeo M, Scardapane A, Sabbà C. Liver involvement in a large cohort of patients with hereditary hemorrhagic telangiectasia: echo-color-Doppler vs multislice computed tomography study. J Hepatol. 2008;48:811-20. , 6666. Buscarini E, Danesino C, Olivieri C, Lupinacci G, Zambelli A. Liver involvement in hereditary haemorrhagic telangiectasia or Rendu-Osler-Weber disease. Dig Liver Dis. 2005;37:635-45. ]. In the majority, these will remain asymptomatic. However, in a subset of patients with HHT, pulmonary hypertension can occur via two mechanisms. Most commonly, extensive arteriovenous fistulae develop between the abdominal arterial circulation (normally the hepatic artery) and the portal or hepatic venous system, causing high output heart failure [6767. Garcia-Tsao G, Korzenik JR, Young L, Henderson KJ, Jain D, Byrd B, Pollak JS, White RI Jr. Liver disease in patients with hereditary hemorrhagic telangiectasia. N Engl J Med. 2000;343:931-6. , 6868. Garcia-Tsao G. Liver involvement in hereditary hemorrhagic telangiectasia (HHT). J Hepatol. 2007;46: 499-507. ] with elevated left ventricular diastolic pressure (but typically preserved left ventricular systolic function) and secondary pulmonary hypertension with normal or low pulmonary vascular resistance, normal transpulmonary gradient (the difference between the mean pulmonary artery pressure and left atrial pressure >12 m HG) and high transpulmonary flow. In the much less common form of pulmonary hypertension, a pulmonary vasculopathy develops similar to that seen in primary pulmonary hypertension characterised by an elevated pulmonary vascular resistance and transpulmonary gradient and a normal left ventricular diastolic pressure (the cardiac output is typically normal or reduced). When fistulae occur between the hepatic or intestinal arterial circulation and the hepatic vein, hepatic encephalopathy and hepatic ischaemia have been reported [6767. Garcia-Tsao G, Korzenik JR, Young L, Henderson KJ, Jain D, Byrd B, Pollak JS, White RI Jr. Liver disease in patients with hereditary hemorrhagic telangiectasia. N Engl J Med. 2000;343:931-6. , 6868. Garcia-Tsao G. Liver involvement in hereditary hemorrhagic telangiectasia (HHT). J Hepatol. 2007;46: 499-507. , 6969. Larson AM. Liver disease in hereditary hemorrhagic telangiectasia. J Clin Gastroenterol. 2003;36:149-58. ]. Portal hypertension can be seen with fistulae between the intestinal or hepatic arterial circulation and the portal vein [6767. Garcia-Tsao G, Korzenik JR, Young L, Henderson KJ, Jain D, Byrd B, Pollak JS, White RI Jr. Liver disease in patients with hereditary hemorrhagic telangiectasia. N Engl J Med. 2000;343:931-6. , 6868. Garcia-Tsao G. Liver involvement in hereditary hemorrhagic telangiectasia (HHT). J Hepatol. 2007;46: 499-507. ]. When high output heart failure is a prominent feature, medical therapy (diuretics, maintenance of a haemoglobin >10 g/dl, maintenance of sinus rhythm, iron replacement) frequently allows significant symptomatic improvement. If this is insufficient, percutaneous fistula closure should be considered when it is technically feasible. In some cases a selective percutaneous approach is not helpful, particularly with diffuse multiple fistulae in which case hepatic artery embolisation [7070. Chavan A, Caselitz M, Gratz KF, Lotz J, Kirchhoff T, Piso P, Wagner S, Manns M, Galanski M. Hepatic artery embolization for treatment of patients with hereditary hemorrhagic telangiectasia and symptomatic hepatic vascular malformations. Eur Radiol. 2004;14:2079-85.
Very good report on treatment of hepatic malformations encountered in patients with hereditary telangiectasia.] or surgical ligation [7171. Koscielny A, Willinek WA, Hirner A, Wolff M. Treatment of high output cardiac failure by flow-adapted hepatic artery banding (FHAB) in patients with hereditary hemorrhagic telangiectasia. J Gastrointest Surg. 2008; 12:872-6. ] have been performed. However, a non-selective approach is not without risk (potential biliary ischaemia and hepatic necrosis) and in some cases liver transplantation may remain the last resort [7272. Lerut J, Orlando G, Adam R, Sabbà C, Pfitzmann R, Klempnauer J, Belghiti J, Pirenne J, Thevenot T, Hillert C, Brown CM, Gonze D, Karam V, Boillot O; European Liver Transplant Association. Liver transplantation for hereditary hemorrhagic telangiectasia: Report of the European liver transplant registry. Ann Surg. 2006;244:854-62; discussion 862-4. , 7373. Scelzo C, Greco S, Bonanni L, Di Cocco P, D’Angelo M, Laurenzi C, Pisani F, Famulari A, Orlando G. The role of liver transplantation in the treatment of hereditary hemorrhagic telangiectasia: a short literature review. Transplant Proc. 2007;39:2045-7. ].
Hepatic AV fistulae
- The most common feeding artery is the hepatic artery (60%)
- Clinical features include oesophageal varices, ascites, splenomegaly, intestinal or pancreatic ischemia, haemobilia or gastrointestinal haemorrhage. Right heart failure and pulmonary hypertension are uncommon
- Imaging modalities are ultrasound, MRI or contrast CT
- Small asymptomatic fistulae can be managed conservatively with non-invasive imaging follow-up
- Treatment of symptomatic fistulae or asymptomatic fistulae causing portal hypertension is recommended
- Asymptomatic extrahepatic arterioportal fistulae should be considered for closure
- Percutaneous treatment is the first choice in anatomically suited fistulae. Depending on the size and location, coils or vascular plugs can be considered
- Potential complications are liver failure (from liver infarction), portal vein thrombosis, biliary fistulae, stricture formation of stroke
- Accidental hepatic artery embolisation usually does not have any clinical consequences except in a patient with compromised liver function at baseline
Arteriovenous fistulae as a result of percutaneous coronary or peripheral interventional procedures
The reported risk of femoral AV fistulae due to previous femoral arterial and/or venous access is low and varies depending on the method of examination, with an incidence varying from around one in a thousand up to approximately three in one hundred [7474. Glaser RL, McKellar D, Scher KS. Arteriovenous fistulas after cardiac catheterization. Arch Surg. 1989;124: 1313-5. , 7575. Kelm M, Perings SM, Jax T, Lauer T, Schoebel FC, Heintzen MP, Perings C, Strauer BE. Incidence and clinical outcome of iatrogenic femoral arteriovenous fistulas: implications for risk stratification and treatment. J Am Coll Cardiol. 2002;40:291-7.
Landmark article on iatrogenic femoral arteriovenous fistulae. This demonstrates the importance of a conservative strategy for most iatrogenic femoral arteriovenous fistulae., 7676. Perings SM, Kelm M, Jax T, Strauer BE. A prospective study on incidence and risk factors of arteriovenous fistulae following transfemoral cardiac catheterization. Int J Cardiol. 2003;88:223-8. , 7777. Kent KC, McArdle CR, Kennedy B, Baim DS, Anninos E, Skillman JJ. A prospective study of the clinical outcome of femoral pseudoaneurysms and arteriovenous fistulas induced by arterial puncture. J Vasc Surg. 1993;17:125-31; discussion 131-3. ]. In a large recent prospective study, with routine postprocedural auscultation the day after femoral access followed by ultrasonography if a bruit was discovered, the incidence was 0.86% [7575. Kelm M, Perings SM, Jax T, Lauer T, Schoebel FC, Heintzen MP, Perings C, Strauer BE. Incidence and clinical outcome of iatrogenic femoral arteriovenous fistulas: implications for risk stratification and treatment. J Am Coll Cardiol. 2002;40:291-7.
Landmark article on iatrogenic femoral arteriovenous fistulae. This demonstrates the importance of a conservative strategy for most iatrogenic femoral arteriovenous fistulae.]. A higher incidence (2.8%) was reported in a smaller study using routine ultrasound follow-up after femoral access [7878. Kresowik TF, Khoury MD, Miller BV, Winniford MD, Shamma AR, Sharp WJ, Blecha MB, Corson JD. A prospective study of the incidence and natural history of femoral vascular complications after percutaneous transluminal coronary angioplasty. J Vasc Surg. 1991;13:328-33; discussion 333-5. ]. It is probably higher with arteriotomies distal to the common femoral artery bifurcation and with interventional rather than diagnostic procedures. Risk factors are female gender, hypertension, puncture of the left femoral artery (versus the right) and higher intensity anticoagulation [7575. Kelm M, Perings SM, Jax T, Lauer T, Schoebel FC, Heintzen MP, Perings C, Strauer BE. Incidence and clinical outcome of iatrogenic femoral arteriovenous fistulas: implications for risk stratification and treatment. J Am Coll Cardiol. 2002;40:291-7.
Landmark article on iatrogenic femoral arteriovenous fistulae. This demonstrates the importance of a conservative strategy for most iatrogenic femoral arteriovenous fistulae.]. In the largest study to date, the risk was not related to the sheath size and number [7575. Kelm M, Perings SM, Jax T, Lauer T, Schoebel FC, Heintzen MP, Perings C, Strauer BE. Incidence and clinical outcome of iatrogenic femoral arteriovenous fistulas: implications for risk stratification and treatment. J Am Coll Cardiol. 2002;40:291-7.
Landmark article on iatrogenic femoral arteriovenous fistulae. This demonstrates the importance of a conservative strategy for most iatrogenic femoral arteriovenous fistulae.]. The connection can be either between the common, deep or superficial femoral artery with the adjacent vein. Most frequently, fistulae are detected on routine follow-up after femoral access by auscultation of a bruit. A significant proportion of AV fistulae (nearly 40% in one study) have closed spontaneously at follow-up [7575. Kelm M, Perings SM, Jax T, Lauer T, Schoebel FC, Heintzen MP, Perings C, Strauer BE. Incidence and clinical outcome of iatrogenic femoral arteriovenous fistulas: implications for risk stratification and treatment. J Am Coll Cardiol. 2002;40:291-7.
Landmark article on iatrogenic femoral arteriovenous fistulae. This demonstrates the importance of a conservative strategy for most iatrogenic femoral arteriovenous fistulae.]. Most spontaneous closures occur within the first month after access and almost all within the first year. Larger fistulae (shunt volume of >400 ml/min) are less likely to close spontaneously. Spontaneous closure may also be less likely with continued anticoagulation. The overwhelming majority are asymptomatic and can be managed conservatively. In 88 patients found to have fistulae after femoral access, none developed symptoms [7575. Kelm M, Perings SM, Jax T, Lauer T, Schoebel FC, Heintzen MP, Perings C, Strauer BE. Incidence and clinical outcome of iatrogenic femoral arteriovenous fistulas: implications for risk stratification and treatment. J Am Coll Cardiol. 2002;40:291-7.
Landmark article on iatrogenic femoral arteriovenous fistulae. This demonstrates the importance of a conservative strategy for most iatrogenic femoral arteriovenous fistulae.]. Hence, rarely do iatrogenic femoral AV fistulae need to be treated. However, symptoms related to a fistula can occur. In this context, high output heart failure and unilateral lower extremity oedema have been reported as well as degenerative aneurysmal arterial dilatation and limb ischaemia [7474. Glaser RL, McKellar D, Scher KS. Arteriovenous fistulas after cardiac catheterization. Arch Surg. 1989;124: 1313-5. , 7979. Sako Y, Varco RL. Arteriovenous fistula: results of management of congenital and acquired forms, blood flow measurements, and observations on proximal arterial degeneration. Surgery. 1970;67:40-61. , 8080. Shumacker HB Jr. Aneurysm development and degenerative changes in dilated artery proximal to arteriovenous fistula. Surg Gynecol Obstet. 1970;130: 636-40. , 8181. Kron J, Sutherland D, Rosch J, Morton MJ, McAnulty JH. Arteriovenous fistula: a rare complication of arterial puncture for cardiac catheterization. Am J Cardiol. 1985;55:1445-6. , 8282. Schaub F, Theiss W, Heinz M, Zagel M, Schomig A. New aspects in ultrasound-guided compression repair of postcatheterization femoral artery injuries. Circulation. 1994;90:1861-5. , 8383. Lemaire JM, Dondelinger RF. Percutaneous coil embolization of iatrogenic femoral arteriovenous fistula or pseudo-aneurysm. Eur J Radiol. 1994;18:96-100. ]. Heart failure related to left to right shunting at the interatrial or interventricular level generally does not develop with shunts <30% of the cardiac output. Therefore, high-output heart failure or signs of right ventricular volume overload do not usually occur at fistula flow volumes of less than 500 ml/min. Flow volumes of greater than 500 ml/min are rare. The diagnosis and flow volume quantification can easily be made by femoral arterial ultrasound. This typically demonstrates a characteristic continuous unidirectional velocity signal when positioning the Doppler signal in alignment with the fistula tract. In contrast to the frequently successful ultrasound-guided compression of pseudoaneurysms, this is often unsuccessful in AV fistulae due to the need for anticoagulation or double antiplatelet therapy related to a previous interventional procedure. In addition, the tract is frequently too large or too short to achieve cessation of flow. Coil embolisation is safe only in the rather uncommon long fistula tract. Under the rare circumstance that a femoral AV fistula requires treatment, when the location is distal to the common femoral artery bifurcation and the landing zone with respect to the common femoral bifurcation is long enough, stent graft implantation is a good option [8484. Ruebben A, Tettoni S, Muratore P, Rossato D, Savio D, Rabbia C. Arteriovenous fistulas induced by femoral arterial catheterization: percutaneous treatment. Radiology. 1998;209:729-34. , 8585. Thalhammer C, Kirchherr AS, Uhlich F, Waigand J, Gross CM. Postcatheterization pseudoaneurysms and arteriovenous fistulas: repair with percutaneous implantation of endovascular covered stents. Radiology. 2000; 214:127-31. , 8686. Baltacioglu F, Cimsit NC, Cil B, Cekirge S, Ispir S. Endovascular stent-graft applications in latrogenic vascular injuries. Cardiovasc Intervent Radiol. 2003;26:434-9. ]. In this position, stent injury from hip flexion is likely to be low. For placement, contralateral access is obtained and a cross-over sheath placed with the tip close to the location of the fistula. Road mapping and precise imaging prior to stent deployment are essential. Though, a self-expanding stent (particularly the newer generation stents less likely to migrate on deployment) is an option, these stents are frequently longer than necessary for fistula coverage. The shortest currently available self-expandable stent graft is 25 mm long Viabahn® (W.L. Gore, Flagstaff, AZ, USA). Precise positioning of balloon expandable stents may be easier. For this purpose, the JoStent Graftmaster® (Abbott Vascular Instruments, Deutschland GmbH, Rangendingen, Germany) or the iCast stent™ (Atrium Medical Corporation, Hudson, NH, USA) are available. The former is delivered over a 0.014 inch guidewire and requires a minimal inner diameter of the delivery catheter of 0.74 inch (i.e., at least a 7 Fr guiding catheter or 6 Fr sheath). The latter is delivered over a 0.035 inch guidewire and requires a 6 Fr or a 7 Fr delivery system, depending on the stent diameter. When the position is suboptimal for percutaneous therapy (at the common femoral artery or too close to the bifurcation) surgical therapy should be considered. However, this is accompanied by a not insignificant risk of infection and haemorrhage (due to the high venous pressure).
Arteriovenous fistulae as a result of percutaneous coronary or peripheral interventional procedures
- The incidence of AV fistulae after femoral artery catheterisation varies depending on the diagnostic modality: 1% with clinical auscultation and 3% with systematic ultrasound screening
- Risk factors are female gender, hypertension, left femoral (versus) right femoral access and anticoagulation
- Most fistulae are asymptomatic. Forty percent of fistulae close spontaneously. Most spontaneous closures occur within the first month of the procedure. Large fistulae and those patients on anticoagulation are less likely to close spontaneously
- Ultrasound is the imaging modality of choice. This demonstrates a continuous unidirectional velocity signal in the fistula tract
- Ultrasound compression frequently fails to obliterate the fistula. Symptomatic fistulae, particularly those which cause right heart failure should be considered for closure
- If the landing zone permits (enough distance of the fistula tract from the femoral bifurcation), a covered stent would be an option. Rarely, the fistulous tract is small and long enough to allow coil embolisation
Imaging
Depending on the location, fistulae can be visualised either with ultrasound, CT or MRI. The typical findings on Duplex ultrasonography are a low resistance flow pattern in the feeding artery proximal to the fistula and a high resistance pattern in the feeding artery distal to the fistula. The venous flow pattern at the connecting tract will have the same appearance as an arterial waveform. Occasionally, colour signals in the tissue surrounding the vein, a colour “bruit”, can be seen. The characteristic finding on contrast CT or MRI angiography is venous enhancement in the arterial phase.
Imaging
- The imaging modalities used to identify and characterise an AV fistula are ultrasonography-imaging, CT-imaging or MRI imaging
- Typical findings on ultrasound are a low resistance flow pattern in the feeding artery proximal to the fistula and
- Typical findings on CT or MRI imaging are venous enhancement in the arterial phase
Coils, vascular plugs and gel foam
Coils are the most frequently used device for embolisation. They are generally conveyed via a delivery catheter and placed within the target vessel by a pusher wire. The size of most coils is typically described in the following manner: the first number clarifies the thickness in thousands of an inch, the second the total extended length in centimetres and the third the diameter of the unconstrained coil in millimetres. For example, an 18-5-5 coil can be delivered through a catheter that can accommodate a 0.018 inch wire. The extended length of the coil will be 5 cm and the diameter of the unconstrained coil 5 mm. Sizing is very important. Too small a non-constrained diameter is associated with a distal embolisation risk and too large a diameter will prevent natural coiling. Therefore, the best advice would be to choose a non-constrained diameter slightly larger than the target vessel size. Optimally sized coils appear slightly compressed with an irregular contour after deployment ( Figure 1 ). Different types of coils are available. Most are made of stainless steel or nitinol. Some are coated with fibres to increase the thrombogenicity. Coils work not so much by mechanical obstruction of the vessel flow via the coil but rather by endothelial injury and the material itself both promoting thrombus formation. Delivery occurs via a delivery catheter and by using either the straight end of a suitable conventional guidewire or a pusher wire specifically designed for this purpose. Controlled release detachable coils are now available. This allows retrieval of the coil prior to detachment if the sizing appears inappropriate. It is very important to ensure good guide catheter positioning within the target vessel prior to coil delivery to avoid catheter dislodgment during delivery and embolisation in an unintended vessel. Hydrophilic or microcatheters are useful for this purpose. Note that not all coils, particularly stainless steel coils, are MRI compatible. The compatibility can usually be clarified with the manufacturer.
Vascular plugs are best used for large or medium sized feeding vessels with a short straight landing zone. The most commonly used plugs are AMPLATZER® Vascular Plugs (AGA Medical Corporation) which are self-expandable, multi-layered bilobed nitinol mesh and are available in different diameters and lengths. The plugs are attached to a delivery wire and can be deployed, resheathed and redeployed. When positioning is optimal, plugs are detached by anticlockwise rotation of the delivery wire with a micro screw mechanism. A plug diameter approximately 30% larger than the target vessel is usually chosen. The device is anchored by its radial force. The older generation plugs required a sheath or larger guide catheter for delivery, however, the latest generation plugs can be deployed via 4 Fr or 5 Fr catheters [8787. Mordasini P, Szucs-Farkas Z, Do DD, Gralla J, Kettenbach J, Hoppe H. Use of a latest-generation vascular plug for peripheral vascular embolization with use of a diagnostic catheter: preliminary clinical experience. J Vasc Interv Radiol. 2010;21:1185-90.
Helpful report on new low profile vascular plugs that can be delivered with small calibre catheters.]. In some cases, vascular plugs can be deployed first and used as a cage for coil embolisation. Four AMPLATZER® Vascular Plugs are currently available ( Figure 8 ). The AMPLATZER Vascular Plug is a single lobe single layer nitinol cage that is optimal for vessel occlusion with short landing zones. There are 7 sizes from an unconstrained diameter of 4 mm to16 mm (unconstrained length of 7-8 mm). It is delivered via a 4-6 F delivery sheath or 5-8 F guide catheter. The AMPLATZER Vascular Plug II is a multi-layered nitinol cage with one disc at the proximal and distal end, respectively (all of which are of the same diameter). Eleven sizes are available with unconstrained diameters of 3 mm to 22 mm (unconstrained lengths of 6-18 mm). Depending on the size, it can be delivered via a 4-8 F sheath or 5-9F guide catheter. The multi-lobed and multi-segmented design may allow more rapid vessel occlusion. The AMPLATZER Vascular Plug III has an elliptical shape and consists of multiple nitinol layers. In addition, it has extended rims that allow more secure anchoring. It is particularly useful for occlusion of oval, rather than round defects (e.g. in cases of paravalvular leaks). Its diameter in the long axis is 4-14 mm and in the short axis 2-5 mm (unconstrained length 6.5 mm) and it can be delivered via 4-7 F sheaths or 6-9 F guide catheters. The AMPLATZER Vascular Plug IV is a single layer bi-lobed nitinol cage that has a very low profile and can be delivered via some (0.038 inch compatible) 4 F diagnostic catheters.
Gel foams and liquid embolic agents though commonly used for tumour embolisation, are rarely used for fistula occlusion given the significant risk of distal embolisation.
Coils, vascular plugs and gel foam
- Coil sizing is paramount to the success of coil embolisation. The non-constrained diameter should be slightly larger than the feeding vessel diameter
- Controlled release coils allow easy retrieval prior to deployment. Hydrophilic catheters for coil delivery are useful
- Not all coils are MRI compatible
- Vascular plugs are used for large feeding vessels. A plug diameter 30% larger than the diameter of the feeding vessel is recommended
- Some later generation plugs can be delivered via 4 Fr or 5 Fr catheters
Conclusions
Arteriovenous fistulae are uncommon. Moreover, fistulae requiring treatment are rare. Management depends on symptoms, size and haemodynamic impact and needs to be tailored to the organ involved. Most frequently, the treatment of choice is percutaneous closure of the fistula or feeding vessel. Though the devices used for fistula occlusion are easily deployed, access to the target artery and device delivery, as well as sizing, require skill and significant operator experience coupled with versatility and familiarity with the management of complications, particularly retrieval of embolised material (which is discussed elsewhere). Though prospective randomised data examining the effectiveness and clinical benefit of fistula closure does not exist, the immediate anatomical result and physiological improvement are frequently readily apparent and, provided the appropriate patient is selected, can be expected to translate into a clinical benefit.
Personal perspective - Peter N. Ruygrok
Though percutaneous treatment of AV fistulae is tempting, particularly if the anatomy is well suited to this approach, it is important to remind oneself that a substantial number of fistulae (e.g., most coronary fistulae after myocardial biopsies and some iatrogenic femoral fistulae after femoral access) are better left alone and can resolve. Likewise, though small and frequently initially clinically silent, some fistulae (particularly pulmonary AV fistulae) require a more aggressive strategy to prevent their potentially devastating consequences. Collaboration and a team approach with specialists who are familiar with the organ harbouring the fistula and its vascular territory is paramount in making the best treatment decision.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}